This article describes the complex dental treatment of an adult patient with multiple missing teeth, mild chronic periodontitis, and a malocclusion with a cant of the occlusal plane. After periodontal treatment, titanium implants and a miniscrew were placed to correct the occlusal plane canting with orthodontic treatment. Prosthodontic treatment was completed by using osseointegrated implants to replace the missing teeth.
In adult patients, the loss of teeth or periodontal support can cause pathologic migration of a single tooth or a group of teeth. This can result in the development of a median diastema or general spacing of the teeth with or without incisor proclination, rotation, or tipping of premolars and molars and collapse of the posterior occlusion with decreasing vertical dimensions. Treatment is complicated in patients with many missing and periodontally compromised teeth. The primary objective of periodontal therapy is to restore and maintain the health and integrity of the attachment apparatus of the teeth. Adjunctive orthodontic therapy is necessary to solve these problems and can facilitate management of several restorative and esthetic problems or difficulties relating to fractured teeth, tipped abutment teeth, excess spacing, inadequate pontic space, malformed teeth, hypererupted incisors, and diastema.
Fortunately, implants in edentulous areas can provide orthodontic anchorage and later serve as prosthetic abutments. Implants are particularly helpful when many posterior teeth are missing and the teeth must be moved in 1 direction. The benefit of implants is that, when several teeth are missing, the reciprocal effects of conventional methods can be minimized. Miniscrew implants have also been used successfully.
A LeFort I osteotomy with asymmetric maxillary impaction is often used to correct the cant of the maxillary occlusal plane. However, canting caused by extruded teeth can be corrected easily with conventional orthodontic appliances and skeletal anchorage. This correction occurs through intrusion of the extruded teeth on 1 side of the maxilla, thereby avoiding a more involved surgical approach.
Diagnosis and etiology
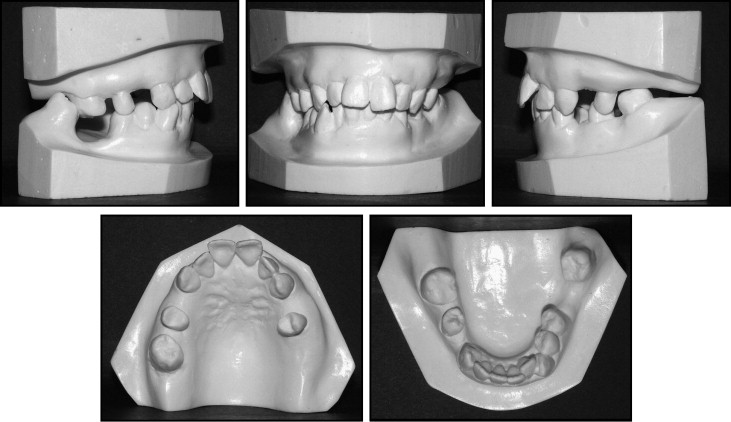
A 43-year-old woman had lost several teeth and was unsatisfied with the esthetic and functional aspects of her dentition ( Figs 1-3 ). She also wanted to maintain her natural teeth and improve esthetics and function.

A thorough examination, which included mounted diagnostic casts, was performed. The patient had a mixed dental-skeletal malocclusion. The vertical dimension of the occlusion appeared to be decreased, secondary to multiple missing posterior teeth and vertical overclosure, but she had an excessive vertical facial height.
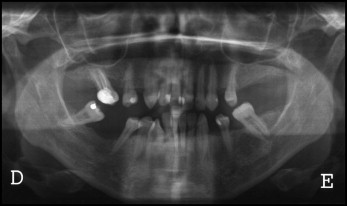
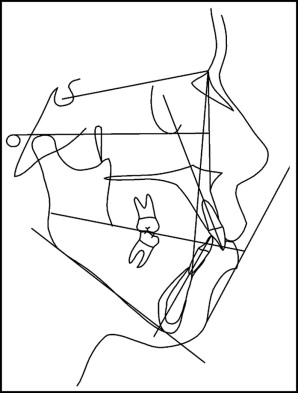
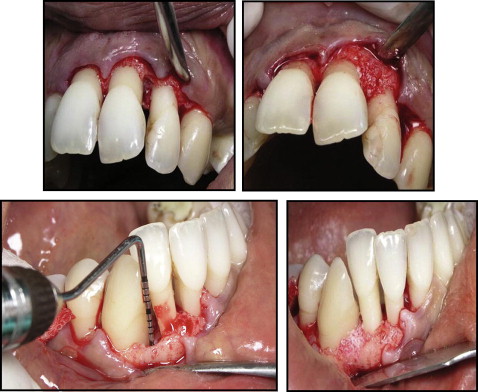
The following diagnosis was established as a result of the clinical and radiographic examinations: Class II Division 1 malocclusion with maxillary incisor protrusion, high mandibular plane angle with vertical overclosure ( Figs 4 and 5 ), chronic mild periodontitis ( Figs 6 and 7 ), partially edentulous maxilla and mandible, and a canted occlusal plane. Her mandible was shifted to the right, and there was unilateral extrusion of the teeth on the maxillary and mandibular left sides. Her asymmetry was accentuated by this extrusion ( Fig 8 ).


The mandibular midline was shifted 1 mm to the right of the midsagittal plane. No tooth size-arch length discrepancy was present in either arch. Both left and right canines were in a Class II dental relationship ( Fig 3 ).
Treatment objectives
The following treatment objectives were established for this patient: (1) treatment of her periodontal disease, (2) reestablishment of the correct occlusal plane, (3) improvement of smile asymmetry by intrusion of the maxillary left anterior teeth; and (4) dental implants and prosthetic rehabilitation of the posterior occlusion.
Treatment objectives
The following treatment objectives were established for this patient: (1) treatment of her periodontal disease, (2) reestablishment of the correct occlusal plane, (3) improvement of smile asymmetry by intrusion of the maxillary left anterior teeth; and (4) dental implants and prosthetic rehabilitation of the posterior occlusion.
Treatment alternatives
Based on the objectives, we could have chosen to reconstruct the occlusal plane by combined orthodontic and surgical treatment with maxillary impaction surgery (more in the left side) and mandibular rotation with advancement. However, the risks and the treatment costs would have been high, and the patient was reluctant to undergo surgery. She was willing to accept a compromise result, because she was more concerned about her dental problems and periodontal health than her facial appearance. Also, the surgery would not necessarily improve the periodontal problems.
Treatment progress
After the diagnostic workup was completed, a treatment plan was developed by using a team approach with orthodontics, periodontics, oral surgery, and prosthodontics. The initial treatment plan involved determination of which teeth were essential for prosthodontic treatment and which teeth had a hopeless periodontal prognosis or were not essential to the overall treatment.
The manbibular right second premolar was scheduled for extraction because of periodontal bone loss and high mobility. Because of a severe lack of bone, the mandibular left second premolar needed endodontic therapy, and a pontic replacement on this side was planned ( Fig 8 ).
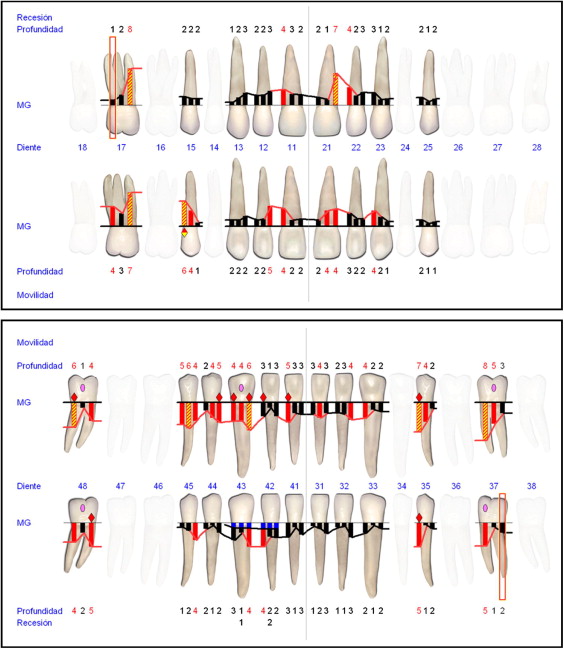
The periodontal disease was treated by nonsurgical and surgical methods ( Fig 7 ). Full-mouth scaling and root planing were performed in 2 appointments. After a 2-month reevaluation period, pocket-depth reduction was achieved in almost every site. The distal face of the maxillary right central incisor and the mesial face of the mandibular left canine probed more than 5 mm with bleeding on probing.
A secondary surgical phase of periodontal treatment was scheduled for both of these sites. Periodontal regeneration of the 2 wall bony defects began by using enamel protein derivative (Emdogain; Straumann, Basel, Switzerland) and hydroxyapatite (Bio-oss; Geistlich, Wolhusen, Switzerland) in the anterior maxillary region and mesially on the mandibular right canine. These sites healed uneventfully before orthodontic treatment was started. Periodontal maintenance visits were scheduled every 3 months during orthodontic treatment.
Orthodontic therapy included intrusion of the left anterior teeth; this leveled the occlusal plane. Anchorage for orthodontic intrusion would be provided by an osseointegrated titanium implant in place of the left first maxillary premolar ( Fig 9 ). Additional titanium implants would also be placed in several other positions after orthodontic alignment ( Fig 9 ). After the malocclusion had been corrected, dental implants would be used for implant-fixed supported prostheses ( Fig 10 ).



