Introduction
Motivation and cooperation are vital components of orthodontic treatment if a good outcome is to be achieved. In this study, we used Q-methodology to investigate motivating factors among adolescents seeking orthodontic treatment and parents wanting their children to undergo orthodontic treatment. This technique asks participants to rank a series of statements, and the analysis of this ranking then provides insight into the participants’ opinions.
Methods
Each of these complementary studies was divided into 2 phases: interviews to generate a list of reasons for seeking orthodontic treatment and the use of Q-methodology to assess and categorize the relative importance of these reasons for the groups of participants. In the patient study, 32 items were generated from the interviews and placed in order of importance on a Q-methodology grid by 60 patients who were about to commence orthodontic treatment. The rankings were subjected to factor analysis, which categorized the patients’ views into groups of shared opinions. The same methodology was used with the parent group, and a Q-methodology grid was designed to accommodate 35 items that were then ranked by the 60 parents. The rankings were subjected to factor analysis as for the patient group.
Results
For the patients, factor analysis identified 3 factors, all of which included esthetics, as important. The remaining respondents had more individual viewpoints and did not map to any of the 3 factors. For the parents, factor analysis identified 4 factors, all of which included treatment in adolescence to prevent future problems, as important.
Conclusions
This study showed that Q-methodology is a novel and efficient tool that can be used in dental research with few difficulties. It might prove useful for the aspects of care for which subjective views or opinions play an important role.
Many factors motivate children and their parents to seek orthodontic treatment. Ascertaining this motivation and maintaining it throughout treatment is crucial if successful outcomes are to be achieved. When motivation is lost, there is a danger that a patient’s compliance will suffer, and this might lead to premature termination of treatment or a compromised result. Various techniques have been suggested to predict and enhance compliance in new patients, but this has repeatedly been shown to be difficult.
There are many reasons that adolescents undergo orthodontic treatment. However, it appears that the desire for a better dental appearance is one of the most important, alongside the advice of the dentist or significant others. An American study of 227 patients and their parents compared participants’ motivation for treatment with their subsequent cooperation. The authors concluded that 93.4% of the children rated esthetic concerns as the most important reason for seeking orthodontic treatment, and they also noted that the higher the patient’s motivation before treatment, the greater their cooperation during treatment appeared to be. Another study that surveyed 207 adolescent patients showed that parents played an important part in decisions regarding orthodontic treatment. The results suggested that parents accounted for 41% of the initial drive for treatment, and the general dentist suggested orthodontic treatment in a third of the referrals.
Trulsson et al used qualitative methodology to establish why adolescents underwent treatment, and data analysis showed 5 descriptive categories: being liked by everyone else, being diagnosed, focusing on the mouth, obeying social norms, and forced decision making. The results showed that external influences played a large part in motivating teenagers to undergo treatment, and these external factors included input from others: referring dentist, family members, and peers. However, the teenagers were not fully conscious of these external influences and often believed that they had made independent decisions to have treatment.
Clearly, parents have a significant role in a patient’s motivation and compliance, and some researchers have shown that parents can actually help clinicians to predict patient compliance. Lewit and Verolainen concluded that the parent’s wish concerning treatment for the child was the most powerful single factor in determining a patient’s motivation for orthodontic treatment.
Q-methodology is a technique that combines qualitative and quantitative approaches to explore subjective issues, such as motivation and compliance, by categorizing subjects based on their opinions or motivations. Q-methodology involves generating a set of opinion statements, usually through interviews or focus groups, and these are then ranked by a different group of people. The final phase of the technique involves a factor analysis to provide insight into a participant’s opinions. The use of Q-methodology is limited in dentistry, but it has long been used in social sciences and more recently also in medicine. Only 2 examples of its use in orthodontics were found in the literature, both of which used Q-methodology as a ranking process and did not perform factor analysis to identify different group types or themes.
We aimed to use Q-methodology to investigate why adolescents seek orthodontic treatment and to attempt to classify them according to the similarity of their views. In addition, we sought to establish why parents want their children to have orthodontic treatment and to group parents according to similarities in motivation. This is one of the first studies in orthodontics to use Q-methodology, and it is hoped that, if patients and parents can be grouped according to their views, it might be possible to subsequently develop a set of specific motivational strategies. An effective strategy could then be selected for each patient according to the motivational profile that he or she most closely mapped to.
Material and methods
Ethical approval was obtained for the study, and all participants signed a consent form.
Adolescent patients between the ages of 10 and 16 years were included in the study. Those with clefts of the lip or palate, craniofacial syndromes, and potential orthognathic patients were excluded because we thought that they were not representative of the typical orthodontic population.
Parents were asked to participate if they were accompanying new patients between the ages of 10 and 16 years for routine orthodontic consultations. Parents of patients with syndromic conditions or clefts of the lip or palate, or who were referred for orthognathic treatment were excluded from the study. The sample of parents in this study was recruited independently of the patient sample to prevent confounding influences between the groups.
The first part of our study was the interviews. Two researchers (R.P. and S.S.) were trained in the process of in-depth interviewing. One researcher (R.P.) undertook all patient interviews, and the other (S.S.) undertook all parent interviews. The interviews generated a list of reasons why adolescent patients wanted have orthodontic treatment or why parents wanted their child to undergo treatment. The interviews were tape recorded and transcribed verbatim immediately afterward. The transcription and interview analysis were ongoing activities to ensure that the researcher was aware of any emerging themes. When no new themes arose, saturation was said to have been reached, and no further interviews were carried out. The transcripts were analyzed to identify a list of statements pertaining to the reasons for wanting orthodontic treatment; replicate items were removed, and items were then worded appropriately so that all participants could understand them. A Q-methodology grid was constructed for each of the patient and parent groups to hold the exact number of statements generated ( Fig 1 ).
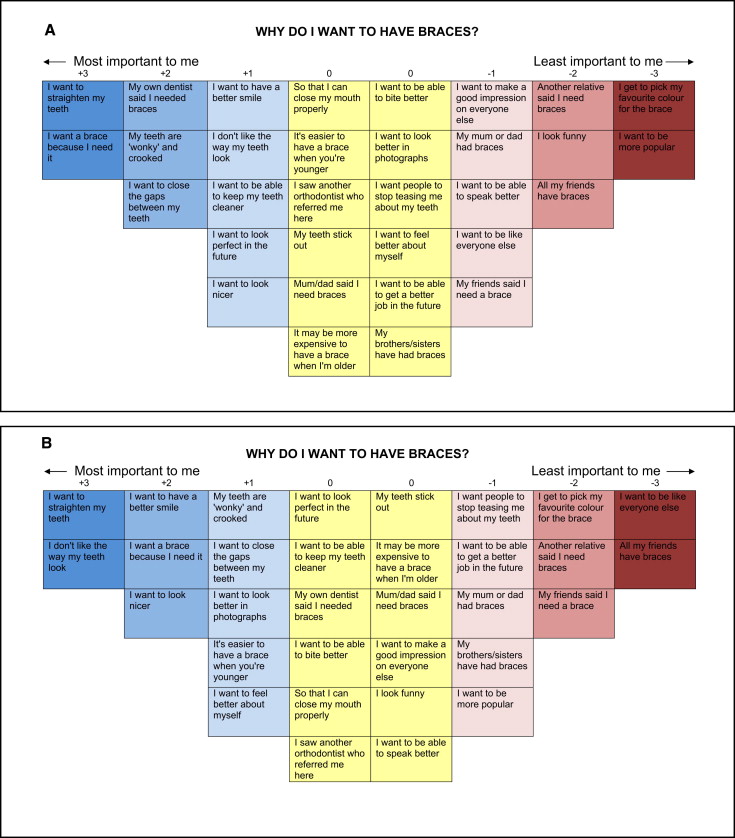
For the patients, 32 items were generated from 11 interviews, and the items were listed on individual cards for placement in the Q-methodology grid. For the parents, 35 items were generated from 13 interviews, and each item was recorded on an individual card to place in the grid.
The second part of the study involved recruitment of 60 new patients and 60 parents by using the same aforementioned inclusion and exclusion criteria. These numbers were in accordance with the study of Shinebourne, who recommended that 40 to 60 participants should be recruited for studies of this type. The participants were initially asked to consider the question, “why do you want to have braces?” (patients) or “why do you want your child to have braces?” (parents), and to read through all the statement cards generated in the first part of the study. They were then asked to place the statements most relevant to them in the far left, positively labeled columns and the statements least relevant to them in the far right, negatively labeled columns. Of the remaining statements, they were then asked to complete the next column by choosing the statements that were most and least relevant to them, respectively. This process was repeated until the remaining statements were placed in the yellow or neutral zone of the board, which included columns all headed with a 0.
The data collected in this manner were recorded and entered into an SPSS spreadsheet and analyzed with SPSS software (version 17.0; SPSS, Chicago, Ill).
Statistical analysis
Global average distribution grids were created for both cohorts by calculating the average score that each statement received, ordering the statements from the one with the highest score to the one with the lowest score, and placing them into the grid in that order (ie, the statement with the highest score was placed in the far left column and the one with the lowest score in the far right column).
Factor analysis involves taking a large set of variables and reducing the data to a smaller set of factors. Data analysis was undertaken to allow a correlation matrix of the participants to be generated and also an unrotated factor matrix with eigenvalues identified. Eigenvalues reflect the amount of variation accounted for by the corresponding factor; an eigenvalue higher than 1 is considered significant. All factors that were considered significant were then rotated (varimax method) to clarify their structure and to maximize the variance between each factor. The participants’ responses were then correlated to indicate who closely mapped to each factor. Only factors with 6 or more people mapping to them were used, and a composite Q-sort was created for each of these factors. These Q-sorts reflect an overall Q-grid for the typical participant profile who loads to that particular factor.
Results
Of the 60 patients recruited for the second part, 63.3% were female, 65% were white, and their mean age was 12.5 years. In the parent group, the female-to-male ratio was 2:1, and there was a slightly higher number of white people than other races (56.7% and 43.3%, respectively). The mean age of the children whose parents participated was 13 years 2 months, and the sex distribution of the children was almost equal (46.7% girls, 53.3% boys).
Figure 1 illustrates the global average distribution grids before factor analysis for girls and boys separately. Generally, the patients sought treatment because they wanted to improve the alignment of their teeth and were dissatisfied with their dental appearance. The 22 boys were motivated to seek treatment because they wanted to improve the alignment of their teeth and because they thought that treatment was necessary. The 38 girls wanted to enhance their dental alignment and viewed their current dental appearance as unsatisfactory.
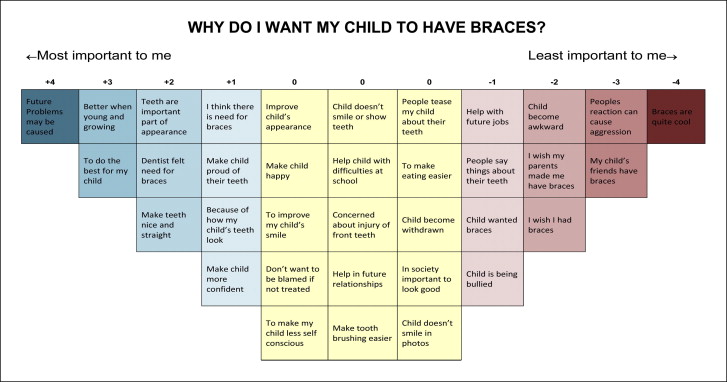
Figure 2 illustrates the average distribution grid for the parents before factor analysis. Since there was little difference between the mothers’ and fathers’ responses, only 1 grid is shown. The statement that received the highest average score was “Future problems might be caused if my child does not get treatment,” and the second statement also recognized the importance of treatment timing. Of the remaining statements in the “most important” zone (ie, the blue zone), 2 described the need for treatment, and 3 described esthetics.
The end point of any Q-methodology study is the summarizing of views emerging from the interpretation of the factors; these are described for the patients and the parents separately.
In the patients’ factor analysis, the unrotated factor matrix identified 15 factors with eigenvalues above 1.0. However, after rotation, the extraction of the top 3 factors provided the clearest solution ( Table I ). The titles given to each factor broadly describe the opinions expressed in that factor. Eleven patients mapped to factor 1 named “esthetics and social acceptance,” and most of the statements related to esthetics, although there were also items related to improving social image. Nine patients mapped to factor 2 (“esthetics and perceived need”), which included statements related to practical needs; however, there were also concerns regarding esthetics and opinions of family members. Seven participants mapped to factor 3, and the statements in this factor related primarily to self-esteem and esthetics, hence the title “esthetics and self-esteem.”
| Factor 1 | Factor 2 | Factor 3 | |
|---|---|---|---|
| +3 | I want to straighten my teeth | I want to close the gaps between my teeth | I want to feel better about myself |
| +3 | I don’t like the way my teeth look | I want a brace because I need it | My teeth stick out |
| +2 | I want to have a better smile | I want to have a better smile | I want to look perfect in the future |
| +2 | My teeth are ‘wonky’ and crooked | I want to straighten my teeth | I want to look nicer |
| +2 | I want to look better in photographs | I want to be able to get a better job in the future | I want to close the gaps between my teeth |
| +1 | I want to look nicer | I want to be able to speak better | I want to be able to get a better job in the future |
| +1 | I want to be like everyone else | I want to be able to keep my teeth cleaner | I want to be able to bite better |
| +1 | I want to be more popular | Another relative said I need braces | I don’t like the way my teeth look |
| +1 | I want to be able to keep my teeth cleaner | I saw another orthodontist who referred me here | I want to have a better smile |
| +1 | I want to be able to get a better job in the future | My brothers/sisters have had braces | It may be more expensive to have a brace when I’m older |
In the parents’ factor analysis, the unrotated factor matrix identified 14 factors with eigenvalues greater than 1; the rotated component matrix showed that only 4 factors had 6 or more parents mapping to them and were therefore considered important ( Table II ).
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | |
|---|---|---|---|---|
| +4 | Future problems may be caused if my child does not get treatment | I think treatment is better now, while he/she is young and still growing | Our dentist thought that my child needed braces | To make my child happy |
| +3 | To make eating easier | To make my child’s teeth look nice and straight | I think my child needs braces | I want to make sure I do the best for my child |
| +3 | To make my child less self-conscious | To make my child less self-conscious | Future problems might be caused if my child does not get treatment | Braces are quite cool these days |
| +2 | I am concerned about my child injuring his/her front teeth | A number of my child’s friends have braces | I think treatment is better now, while he/she is young and still growing | Future problems might be caused if my child does not get treatment |
| +2 | I think treatment is better now, while he/she is young and still growing | Our dentist thought that my child needed braces | I wish my parents made me have braces | To improve my child’s smile |
| +2 | Our dentist thought that my child needed braces | Braces are quite cool these days | To help my child with his/her difficulties at school | To make my child proud of his/her teeth |
| +1 | To help my child with his/her difficulties at school | To improve my child’s smile | To improve my child’s appearance | To make eating easier |
| +1 | My child is being bullied | Because my child doesn’t like to smile and show his/her teeth | People’s reactions to my child’s teeth makes them aggressive and get into fights | To improve my child’s appearance |
| +1 | I want to make sure I do the best for my child | My child wanted braces | Teeth are an important part of a person’s appearance | In today’s society, it is important to look good |
| +1 | Because my child doesn’t like to smile and show his/her teeth | Future problems might be caused if my child does not get treatment | Braces are quite cool these days | To improve my child’s appearance |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


