Fig. 13.1
Residual radicular cyst with an affected tooth

Fig. 13.2
CT Dentascan shows the presence of a cortical erosion
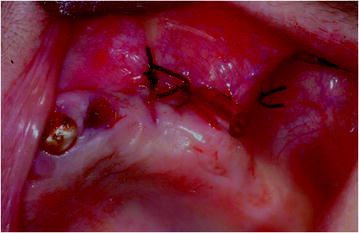
Fig. 13.3
Marsupialization of the cyst and positioning of a drainage tube

Fig. 13.4
Check-up after 6 months
This type of surgery should ideally be performed on soft tissues only. It is therefore crucial to analyze the bone approach surrounding the cyst with imaging techniques, such as traditional computed tomography (CT) or cone beam CT, to correctly view the presence and location of the bone erosion as a surgical access route (Figs. 13.5, 13.6, 13.7, 13.8, 13.9, 13.10).

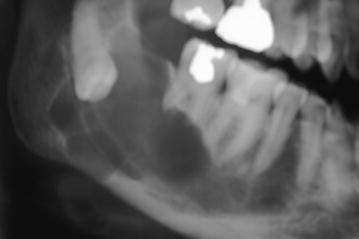
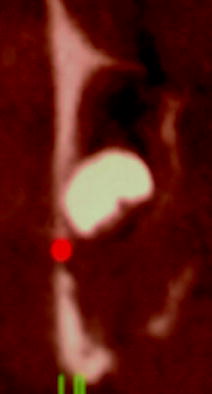
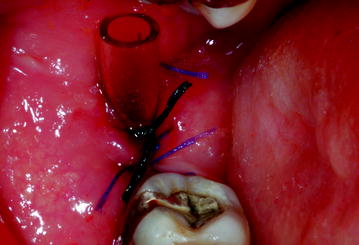


Fig. 13.5
Pericoronal cyst at the level of the crown
Fig. 13.6
Orthopantomography shows a clear resorption of the apex of the crowns
Fig. 13.7
CT Dentascan reveals erosion of the high cortical bone
Fig. 13.8
Marsupialization of the cyst and positioning of a drainage tube
Fig. 13.9
One year after marsupialization, the lesion persists
Fig. 13.10
Orthopantomography one year later shows a bone neoformation inside the cystic cavity and an apical migration
As in the case of dental extraction, antibiotic therapy is equally recommended for marsupialization.
13.2.2 Apicoectomy
When endodontic therapy is not sufficient to treat a chronic apical granulomatous inflammatory process, an apicoectomy of the tooth can be performed, as long as the radiographic examinations confirm the presence of a fenestration of the cortical bone at the level of the root apex to be treated. It is paramount that the oral-hygiene protocol described above for tooth extraction is followed and that patients always receive antibiotic therapy (amoxicillin, metronidazole).
Apicoectomy involves lifting an over-periosteal flap, which should be sufficiently wide to allow an adequate view and should extend at least to the previous and to the following tooth. The second phase involves identifying the area of fenestration at the level of the tooth apex, after which apicoectomy can be performed. Dental tissue is removed starting from the apex to the centralization of the radicular foramen within the diameter of the radicular section. This is followed by a retrograde preparation with ultrasonic instruments and subsequent filling. Checking the seal through methylene blue, cleaning the surgical field, and performing a final radiographic control are extremely important concluding procedures. Silk suture should be used to correctly seal the surgical injury and to prevent bacterial contamination.
13.2.3 Debridement
Debridement is a minimally invasive surgical procedure specifically carried out to treat stage 2 lesions. It is used in patients who experience pain in the osteonecrosis area due to an inflammation of the surrounding soft tissues, which appear erythematous and edematous after intraoral examination. This symptom is often the result of an accumulation of dental plaque and tartar above the lesion. Debridement can also be performed when there are thin sharp bone spicules, which can cause lesions by irritating the edge of the tongue. Debridement can be carried out with manual tools, such as curettes, or with ultrasonic scalers, which allow the atraumatic smoothening of sharp edges. Surface cleaning of the necrotic bone tissue improves the condition of the soft tissues surrounding the necrosis and subsequently reduces the patient’s symptoms.
13.2.4 Sequestrectomy
Quite often, BIONJ provokes the formation of a bone sequestrum during maintenance therapy. This is a fragment of necrotic bone tissue that first acquires mobility and then detaches from the surrounding bone. From a biological perspective, a sequestrum is the consequence of the formation of granulation tissue separating the dead bone from the underlying living bone. Detachment may affect only part of the pathological tissue, or it may lead to the removal of the entire necrotic area. In the first case, several osteonecrotic fragments detach. When the whole area detaches from the surrounding bone, there are two possible scenarios: if the underlying tissue is healthy, a progressive and complete re-epithelialization will follow. If the underlying bone is affected by an osteitic process, a relapse will occur, rather than a complete recovery. It should be noted that the presence of healthy mucosa does not necessarily resolve the pathological process (Fig. 13.11, 13.12, 13.13, 13.14).

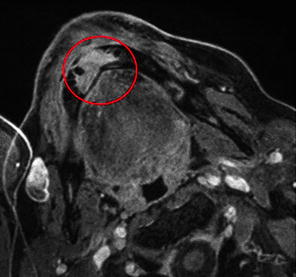


Fig. 13.11
Presence of an osteonecrotic area exposed in zones 41–42
Fig. 13.12
Gadolinium MRI shows the presence of an osteonecrotic area
Fig. 13.13
Spontaneous detachment of an osteonecrotic sequestrum: appearance of gingival tissues. The patient had failed to properly carry out the hygienic routine recommended to every patient at the very beginning of the follow-up cycle and required further instruction to encourage compliance
Fig. 13.14
Osteonecrotic sequestrum
In some cases, after a period of exposure a bone fragment is able to move but it might not be expelled spontaneously. The surgeon’s role is to verify the edges of the sequestrum, using clinical and radiographic examinations (orthopantomography, CT, MRI), and then to remove the bone fragment atraumatically using surgical forceps or Klemmer forceps.
13.2.5 Drug Holiday
Ever since the first reports on BIONJ were published in the literature, the possibility of suspending bisphosphonates has been considered, both as a preventive measure in asymptomatic patients who require maxillofacial surgery and as a therapeutic strategy to verify whether this could somehow stimulate healing of the lesion. Neither is likely realistic in patients treated with intravenous bisphosphonates; these drugs, in fact, are typically used in oncology and play a lifesaving role. By contrast, in most cases, it should be possible to arrange with the prescribing physician a temporary suspension of oral or intramuscular bisphosphonates.
The effectiveness of a drug holiday still needs confirmations by appropriate studies; in the case reports published so far, the results have been encouraging, especially regarding the use of a drug holiday as a preventive measure. These positive findings may be related, at least in part, to the suspension of the anti-angiogenic effect, which allows better wound healing in the mucosa. However, the effects of a drug holiday upon osteoblasts and osteoclasts are still unclear, since bisphosphonates have a long half-life within the bone, such that the effectiveness of a brief suspension of therapy is questionable.
Several authors have attempted to identify objective parameters to predict the risk of osteonecrosis of the jaws. Marx proposed an index measuring the degree of bone remodeling that can be checked frequently and easily, by comparing serum levels before and after a drug holiday [9
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


