Chapter 41 Minimally invasive submucosal glossectomy
1 INTRODUCTION
The major contributing factors to retrolingual collapse in sleep apnea are macroglossia, hypotonia, retrognathia and lingual tonsillar hyperplasia. Any or all of these may contribute to varying degrees in any given individual. All current low morbidity options have limitations in treating the macroglossia component. The ideal procedure for macroglossia would be low morbidity, allow large tissue volume reduction, have low risk of alteration in tongue function and be single stage. Submucosal glossectomy techniques aim to fulfill these criteria, with preservation of mucosa causing minor pain postoperatively. Although the external submucosal glossectomy with hyoid advancement technique discussed in Chapter 47 meets these criteria, disruption of floor of mouth musculature with open dissection (which then must be repaired) is potentially a disadvantage, and is avoidable with minimally invasive techniques.
Critical to safe dissection with limited access is the ability to safely identify vital structures in the tongue. The use of real-time ultrasound to locate the neurovascular bundles (lingual artery and hypoglossal nerve) and guide submucosal dissection was first reported by myself and co-workers in 2003, via a percutaneous approach.1 A bipolar plasma wand (‘coblation’) is used to hemostatically dissect tissue at low temperatures. More recently, several variations of this technique have been used via an intraoral approach, also using coblation and ultrasound guidance. The techniques to be discussed are:
3 OUTLINE OF PROCEDURES
3.1 PERCUTANEOUS APPROACH
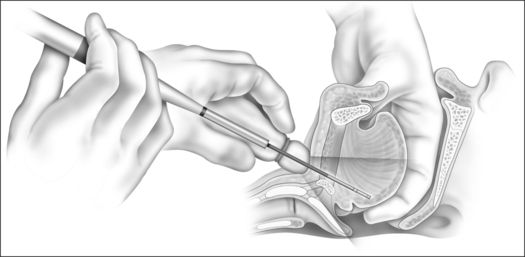
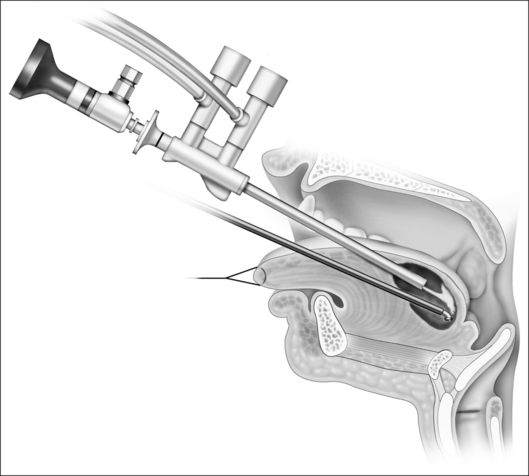
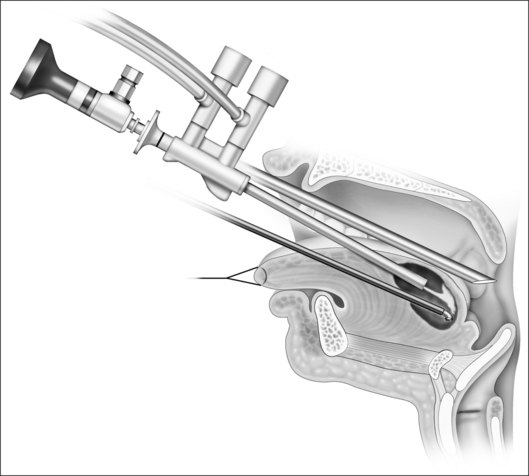
Following induction of general anesthesia, the airway is secured with nasotracheal intubation. Dexametasone and broad-spectrum antibiotic are administered intravenously. Two milliliters of 1% lignocaine+1:100,000 adrenaline are infiltrated in the midline at a level just above the hyoid. An aseptic technique is used with a suprahyoid stab incision, and the surgeon’s dominant hand remains sterile. A bipolar radiofrequency probe is passed into the neck in the midline, while the surgeon’s non-dominant hand palpates the tongue base mucosa intraorally (Fig. 41.1). A mouthguard on the upper teeth protects the surgeon’s knuckles. The probe can be easily felt through the tongue mucosa to determine depth of dissection. Initially a Reflex 55™ wand was used, which was replaced by a Spinevac™ wand. Currently an Evac T&A™ wand is preferred (ENTec division of ArthroCare Corp, Austin, TX, USA). Real-time ultrasound is used throughout the procedure with a Philips (ATL) HDI 5000 SonoCT system and L 12-5 broadband linear array transducer in a sterile cover (Philips Medical Systems, DA Best, The Netherlands), scanning from the neck. A dedicated sonographer is used to simultaneously identify the radiofrequency probe and lingual neurovascular bundles (hypogossal nerve and lingual artery) in the tongue, allowing a minimum of 5mm clearance between the tip of the probe and the bundles at all times. Progressive hemostatic submucosal resection of the tongue base musculature proceeds from 1–2cm above valleculae to foramen cecum (or just anterior to foramen cecum) on power setting seven (for T&A wand), with the depth of treatment gauged by continuous intraoral palpation through intact tongue mucosa and ultrasound guidance. The midline is initially treated, with dissection then carried laterally, to a limited degree, between mucosa and neurovascular bundles.
If intraoperative bleeding occurs, initial management is by ultrasound-guided aspiration of blood and bimanual pressure. In more than 30 of these procedures, I have been able to obtain hemostasis with this method; however, if bleeding were to persist, injection of Floseal® (Baxter International Inc., Deerfield, IL, USA) into the cavity, as suggested by Maturo and Mair,2 or open exploration of the cavity for hemostasis from the neck or dorsal tongue would have been required.
My current preference is for the submucosal lingualplasty approach for tongue reduction (see below).
3.2 INTRAORAL SUBMUCOSAL ENDOSCOPIC ASSISTED APPROACH (‘SMILE’)
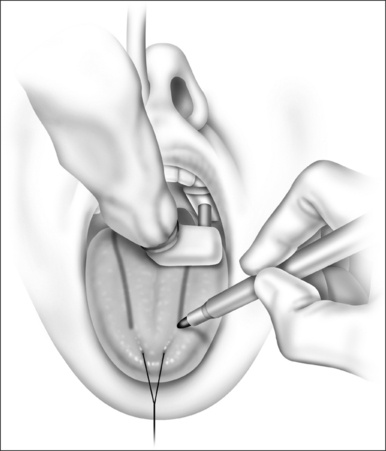
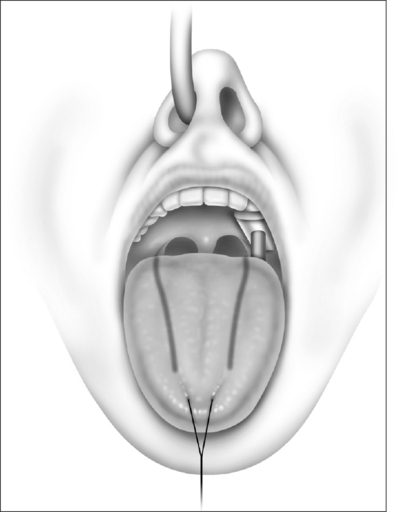
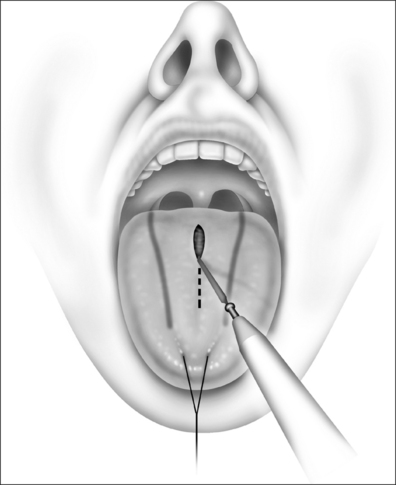
After nasotracheal intubation and general anesthesia, the oral cavity is gently brushed with 0.12% chlorhexidine and a 2-0 silk retraction suture is placed through the anterior midline tongue tip. Intravenous steroid and broad-spectrum antibiotic are given in appropriate pediatric doses. An ultrasound with a ‘hockey stick’ probein a sterile cover then delineates the course of the lingual arteries, which is marked in pen on the dorsal tongue mucosa bilaterally (Figs 41.2 and 41.3). A 1cm midline inci-sion is made approximately 2cm from the tongue tip in pediatric cases, which approximates the junction of anterior and middle thirds of the tongue (anteroposteriorly), and blunt dissection is used to open the incision. An Evac T&A Plasma Wand attached to the Coblator II Surgery System (ArthroCare Corporation, Austin, TX, USA) with coblator ablation at a setting of 9 is then inserted into the incision. Taking care to stay medial to the marked boundaries of the lingual artery, the coblator wand is advanced in a posterior direction, with tissue excised by moving the wand in a superior to inferior fashion. The non-dominant hand palpates the tip of the coblator wand through the tongue mucosa (Fig. 41.4).
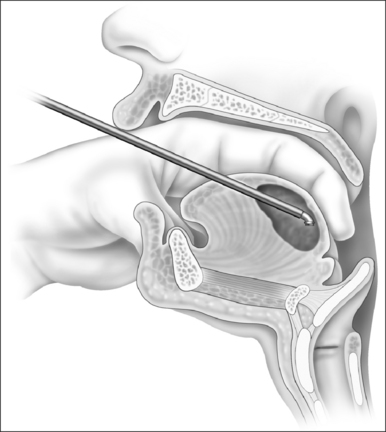
Progress is monitored by intermittently removing the wand and inserting a 0° irrigating endoscope (Clear ESS, SLT, Montgomeryville, PA, USA) into the created cavity. A pressure bag on the saline irrigation of the Clear ESS aids vigorous irrigation of the cavity and therefore identification of bleeding vessels in a clear field. Alternatively, the incision may be extended to allow simultaneous endoscopy and dissection (Fig. 41.5). This facilitates removal of residual strands of undissected muscle, and coagulation of any residual bleeding vessels with the coagulation mode of the wand under endoscopic visualization. I find a second 1cm midline stab incision, 1cmfurther posterior, more convenient for nasendoscope insertion than enlarging the coblator probe incision. This separates the entry points of the nasendoscope and the coblator probe into the tongue, which avoids the instruments crossing, thus avoiding restriction of their movement during dissection.
The light from the nasendoscope in the saline-filledcavity transilluminates the cavity and aids the surgeon in determining the posterior limit of dissection relative tosurface markings, which should be roughly no lower than opposite the tip of the epiglottis. This posteroinferior extent of dissection can be determined by palpation, or visualized by a second 30º or 70º nasendoscope,placed between soft palate and dorsal tongue mucosa to view the epiglottis (Fig. 41.6). The anterior tongue incisionis left open to allow passive drainage of any tissue fluidor blood.
3.3 SUBMUCOSAL MIDLINE GLOSSECTOMY
B. Tucker Woodson has developed a submucosal midline glossectomy technique under local anesthesia, which is described in more detail in the following chapter. In brief, the patient is seated in the operating theater and volun-tarily protrudes their tongue. The initial steps of theprocedure are as for the SMILE procedure, with IV antibiotics and steroids, and marking the location of theneurovascular bundles on the dorsal tongue mucosa with an ultrasound machine and ‘hockey stick’ hand piece using color Doppler mode, covered in a sterile cover (see Figs 41.2 and 41.3).
Local anesthesia and adrenaline infiltration are performed to obtain an anesthetized and vasoconstricted field medial to the marked neurovascular bundles. Any weakness of tongue protrusion warns of infiltrating too close to the neurovascular bundle, and dissection in that area should be avoided. A 5cm midline incision between the anterior and posterior extent of the middle third of the tongue with a Bovie enables direct open access to the tongue musculature (Fig. 41.7). This can be extended into the posterior third of tongue if required.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


