Chapter 52 Maxillofacial surgical techniques for hypopharyngeal obstruction in obstructive sleep apnea
1 INTRODUCTION
Due to poor patient acceptance of tracheostomy and incomplete treatment of obstructive sleep apnea syndrome (OSA) with palatal surgery, we have explored the use of maxillofacial surgical techniques to alleviate hypopharyngeal obstruction.1,2 The aim of surgical treatment is to alleviate upper airway obstruction and its associated neurobehavioral symptoms and morbidities.3,4 No longer is a 50% reduction in the Apnea/Hypopnea Index (AHI) deemed acceptable. Rather, the objective is to treat to cure (normalization of respiratory events and elimination of hypoxemia) and achieve outcomes that are equivalent to those of continuous positive airway pressure (CPAP).5
Selecting the appropriate surgery for a patient can be challenging. However, we have created a two-phase surgical protocol (Powell–Riley protocol) as a logically directed plan to treat the specific areas of upper airway obstruction.6,7 It is imperative that a polysomnogram (PSG) be obtained after any surgery to determine efficacy. Genioglossus advancement and hyoid suspension are considered part of phase I surgery. These are conservative maxillofacial techniques which are often combined with nasal and palatal surgery, should multilevel obstruction exist. Phase II surgery refers to maxillomandibular advancement (MMO). This surgery is usually reserved for those patients who have been incompletely treated with phase I surgery and have documented hypopharyngeal obstruction. MMO is the only surgery which physically creates more room for the tongue by advancing both the mandible and maxilla.
2 PATIENT SELECTION
Proper selection of patients is paramount to achieve successful outcomes and to minimize postoperative complications. The presurgical evaluation requires a comprehensive medical history, head and neck examination, fiberoptic nasopharyngolaryngoscopy, radiographic cephalometric analysis and polysomnography (PSG). This systematic approach will aid in determining the severity of OSA and identifying probable anatomic sites of obstruction. Armed with this information, the surgeon can proceed with a site-specific surgical protocol.8
Since CPAP is considered the primary treatment of OSA, all patients should be offered this therapy prior to surgical intervention. While the efficacy of CPAP has been clearly documented, a subset of patients struggle to comply with CPAP therapy.9 In fact, Kribbs et al. reported that only 6% of patients who receive CPAP therapy are able to tolerate the device for at least 7 hours per night on 70% of days.10
Our protocol encourages all patients to use their CPAP for 2 weeks prior to surgery, particularly those patients with severe OSA (AHI > 40). Preoperative CPAP can alleviate the risks associated with sleep deprivation and postobstructive pulmonary edema. Furthermore, we recommend the insertion of a temporary tracheostomy in patients with an AHI > 60 and/or a SaO2<70% who are intolerant of CPAP.11
Despite a thorough preoperative selection process, it is difficult to accurately predict outcomes for an individual patient. While MMO has documented success rates >90%, our studies have demonstrated that a substantial number of patients may not need such extensive surgery.12–14 In fact, approximately 70% of our patients have obviated the need for MMO by undergoing phase I surgery.12 Thus, we employ conservative maxillofacial surgical techniques (genioglossus advancement or hyoid suspension) to treat hypopharyngeal obstruction, before proceeding to MMO. There are cases in which MMO may be the initial surgery, as in non-obese patients with marked mandibular deficiency and a normal palate.
3 MANDIBULAR OSTEOTOMY WITHGENIOGLOSSUS ADVANCEMENT
When the preoperative evaluation implicates the base of tongue (Fujita Type II–III) as the source of airway obstruction, the genioglossus advancement (GA) procedure is indicated. This procedure is a conservative maxillofacial technique since the osteotomy is created without altering the dental occlusion. The rationale for the GA procedure is to place the primary protrusion muscle of the tongue, the genioglossus, under direct tension. This tension resists the collapse of the tongue into the airway that can occur with sleep-induced hypotonia.15 Essentially, the genial tubercle and the attached genioglossus muscle are advanced anteriorly. The degree of advancement depends on the thickness of the anterior mandible and the compliance of the genio-glossus muscle. Less muscle compliance will provide a greater degree of tension. Unfortunately, there is no objective preoperative study to determine the compliance of the genioglossus muscle.
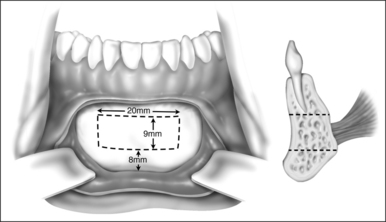
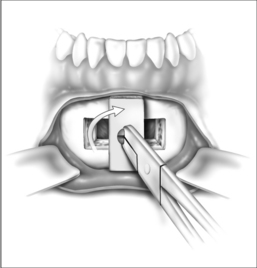
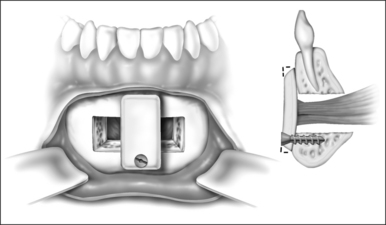
Surgery may be performed under general anesthesia or, in appropriate cases, with the patient under intravenous sedation. An intraoral incision is made in the gingivolabial sulcus, taking care to preserve a cuff of mucosa to facilitate closure and prevent wound dehiscence. The incision extends between the canine dentition. Dissection is performed submucoperiosteally to expose the inferior border of the mandible. The floor of the mouth is palpated to identify the location of the genial tubercle. A rectangular osteotomy is then outlined along the outer cortex of the mandible with a 2-hole sagittal saw blade. The osteotomy is typically 9 mm×20 mm in order to capture the genial tubercle. It is recommended that the superior osteotomy be placed at least 5 mm inferior to the root apices to avoid injury.16 In addition, the inferior osteotomy should be approximately 8 mm above the inferior border of the mandible to avoid a potential fracture (Fig. 52.1). A titanium screw is inserted in the center of the osteotomy to allow manipulation of the fragment (Fig. 52.2). The cuts are then completed through the inner cortex. It is critical to maintain parallel walls while performing the osteotomies to prevent tapering of the inner cortex. The fragment is displaced into the floor of the mouth and hemostasis is achieved (Fig. 52.3). The titanium screw is then grasped and the bony fragment is gently advanced and rotated 90° in either direction (Fig. 52.4). The outer cortex and marrow are removed with the sagittal saw. A 10 mm×2.0 mm titanium screw is used to fix the fragment to the mandible inferiorly (see Fig. 52.4). A pear-shaped cutting burr may be used to contour the bony fragment. Lastly, the wound is irrigated and closed with interrupted absorbable sutures (Fig. 52.5).


4 HYOID MYOTOMY WITH SUSPENSION
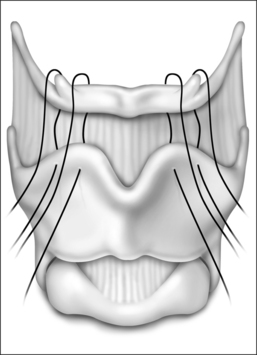
The surgical approach for hyoid suspension is similar to thyroglossal duct excision (Sistrunk procedure). Either general or local anesthesia may be utilized. A horizontal incision is placed at the level of the hyoid bone along a natural skin crease. Dissection is continued to expose the body of the hyoid. The infrahyoid musculature is detached. The stylohyoid ligament may need to be sectioned from the lesser cornu to allow adequate mobility, but the suprahyoid musculature remains intact. The strap muscles are divided in the midline to expose the thyroid cartilage (Fig. 52.6). An Allis clamp is placed on the body of the hyoid and the hyoid complex is advanced anteriorly. Constant traction is maintained on the hyoid bone. Three or four #1-0 permanent sutures are passed around the hyoid and through the superior aspect of the thyroid cartilage to advance and stabilize the hyoid bone (Fig. 52.7). Meticulous hemostasis is achieved. A drain is placed and the wound is closed in layers. Placement of a pressure dressing for 24 hours reduces the incidence of hematoma or seroma formation.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


