Introduction
Our purpose was to study the mechanical properties and phase transformations of orthodontic wires submitted to in-vivo exposure in the mouth for different periods of time.
Methods
Stainless steel wires were tied to fixed orthodontic appliances of 30 patients from the orthodontics clinic of Universidade Federal do Rio de Janeiro School of Dentistry in Brazil. According to the duration of the clinical treatment, the patients were divided into 3 groups. After in-vivo exposure, the samples were studied by mechanical testing (torsion) and ferromagnetic resonance. Statistical analyses were carried out to evaluate the correlation between time of exposure, mechanical properties, and austenite-to-martensite transformation among the groups.
Results
The results were compared with as-received control samples. The torque values increased as time in the mouth increased. The increase in torque resistance showed high correlations with time of exposure ( P = 0.005) and austenite-martensite phase transformation.
Conclusions
The resistance of stainless steel orthodontic wires increases as the time in the mouth increases; this effect is attributed to the austenite-to-martensite transformation.
Austenitic stainless steels are known to undergo a partial transformation to martensite when subjected to plastic deformation. This transformation has been shown to be a function of temperature, microstructure, chemical composition, cumulative strain, and strain rate. However, as far as we know, partial transformation to martensite as a consequence of exposure to the oral environment during orthodontic treatment has not been investigated. Austenitic stainless steels have been used for some decades in orthodontic wires and appliances because of their good combination of mechanical properties and biocompatibility. Orthodontic treatment consists of using and controlling forces acting on teeth and adjacent tissues. Such forces are clinically induced by orthodontic appliances such as wires, brackets, elastics, and springs. Orthodontic treatment results depend on the control of the applied force. Consequently, when designing and preparing each appliance, a clinician must be able to predict its response during treatment. However, the materials are subjected to mechanical actions and the environment in which they function for varying time periods; these can influence clinical behavior. Stainless steels are iron-based alloys that contain chromium and nickel. Chromium improves corrosion resistance, forming a thin, adherent, passive surface chromium oxide layer. When deprived of this protection, stainless steel can suffer strong corrosive attacks. Nickel is responsible for austenite stabilization at room temperature, which increases steel’s toughness. The mechanical properties of materials that must withstand the oral environment are also of concern. Bending the wires into a desired shape causes plastic deformation and induces work hardening, resulting in preferential areas for stress concentration. Complex loading derived from engaging activated wires into bracket slots and masticatory loads is known to exert heavy stresses on the material.
Some reports show that retrieved archwires had much higher fracture incidence than expected from laboratory experiments, which suggested that the archwires would be almost unbreakable. This can be due to several factors, including intraoral aging of wires. This evidence suggests that research approaches with in-vitro methodologies might not adequately model in-vivo phenomena. Despite much evidence from orthodontic materials research, an in-vitro methodology cannot accurately reproduce the complex oral environment. Retrieval analyses provide critical information derived from investigating the performance of the material in vivo. The aim of this study was to characterize the effects of increasing the time of in-vivo exposure in the oral cavity on the mechanical properties of stainless steel archwires.
Material and methods
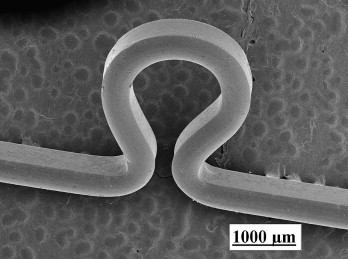
We selected for this study a stainless steel type 304 orthodontic archwire (batch number 0540017, TP Orthodontics, LaPorte, Ind). The wires were straight, 180-mm long, and retangular with an 0.018 × 0.025-in (0.45 × 0.625 mm) cross section. A sample specimen was created by using 40 mm of as-received wire and bending a loop stop about halfway in its length. The height of the loop was 3 mm. The sample was reproduced by using Vision software (Microsoft Corporation, Redmond, Wash) and printed as a real-size template for standardizing the shape of 35 specimens ( Fig 1 ). Part of the wire more susceptible to phase transformation was about 1.0 cm from the central loop; the excess length at the edges allowed for clinical adjustments while tying it to a patient’s appliances.
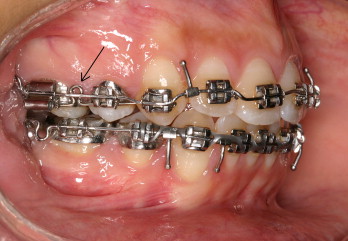
All samples were taken from the same batch of wires and prepared by the same operator (P.P.I) using the same pliers. The 35 specimens were separated in 4 groups (1 control and 3 experimental groups). The control group consisted of 5 specimens of the same size, and equal loop stops and shapes as the experimental ones of as-received wires, having no interaction with the oral environment throughout the trial period. The experimental group consisted of 30 wire specimens that were subjected to the oral environment of 30 patients randomly chosen from the orthodontics clinic of the Universidade Federal do Rio de Janeiro in Brazil. This group was divided into 3 subgroups according to the time of exposure in the mouth: 1, 2, or 3 months. The patients were allocated at random to each subgroup. All participants were undergoing corrective orthodontic treatment, which allowed for specimens to be tied by their edges to the patient’s fixed appliances by using stainless steel 0.010-in (0.24 mm) ligatures and ligature cutters ( Fig 2 ). In all participants, the specimens were placed by the same author (P.P.I.) in the maxillary arch on the right side. This research proposal was approved by the Research Ethics Committee of the Universidade Federal do Rio de Janeiro (number 87/2007). An informed consent form was signed by all 30 patients or their legal representatives. At the end of the clinical period, each experimental specimen was removed with a ligature cutter and tweezers, and placed on a sterile tray with the inner surface that had been turned to the teeth facing up. Before mechanical testing in the laboratory, all experimental and control specimens were placed in an ultrasound cleaner with enzyme detergent Endozyme (DFL, Petrópolis, Rio de Janeiro, Brazil) for 20 minutes. This substance proved ineffective in removing gross debris from the specimens, so the procedure was repeated with a multiuse detergent (Amway, Ada, Mich) for 1.5 hours. After in-vivo clinical time, all samples were subjected to mechanical torque testing.
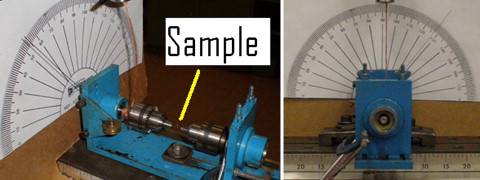
Torque testing is a simple mechanical test. The test consists of twisting a specimen at a defined rate to a prescribed strain or twist, to failure or angle. Figure 3 shows the torque testing device developed by our research team. This apparatus held a specimen by both ends, with 5 mm of wire from the central loop. One end was fixed, and the other was free to rotate, connected to a universal testing machine with a load cell of 50 N (DL10.000, EMIC, Sao José dos Pinhais, Paraná, Brazil). The force required to twist specimen by 15° in torsion was measured. The twist was done at a constant speed of 100 rpm. A 10-cm long rectangular stainless steel wire with a cross section of 0.018 × 0.025 in (0.45 × 0.625 mm) was fixed to the rotating axis, serving as a pointer. A conventional protractor was scanned, printed, and positioned behind the experimental setup; as testing began, the pointer turned, and the test was stopped after a 15° displacement, when force readings were taken in gram-force (gf) units. The output data was force (gf) against twist. But, in principle, the torsion test data are torque-twist curves. To convert the results to torque (gf.mm), the force (gf) readings were multiplied by the radius of the rotating axis (5 mm) and registered in a Microsoft Excel spreadsheet (Microsoft) in gf per millimeter units (gf.mm).
The torsion test simulated the most common clinical situation, when we apply torque in a rectangular orthodontic archwire during the last treatment phase. The orthodontic arch of the last stage has loop or omega in the region of molars. The tested samples were fixed in the region of the molars of the orthodontic appliances. The sample design simulated the region of the archwire, which normally receives torque in the final stage of orthodontic treatment.
In this study, complete data of all parameters, including descriptive statistics and statistical models, were evaluated. The mechanical and magnetic properties results were analyzed with SPSS statistical software (version 13, SPSS, Chicago, Ill). An alpha level of 0.05 was chosen to determine the statistical significance. Post-hoc multiple comparisons were performed by using Bonferroni adjustments for significant tests.
First-derivative ferromagnetic resonance (FMR) spectra were recorded at room temperature and 9.50 GHz by using a Varian E-12 spectrometer with 100-kHz field modulation (Varian, Inc., Santa Clara, Calif). FMR line intensity was computed by double integration of the first derivative absorption spectrum.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


