Introduction
Palatal expansion has been a popular and proven technique for transverse discrepancies used in orthodontics for decades. The short-term effectiveness of the technique is understood, yet questions remain regarding the long-term stability, with much debate surrounding the optimum treatment timing to initiate expansion for the most beneficial and stable results, especially with regard to mixed dentition treatment. The purpose of this study was to determine the long-term stability of palatal expansion performed in the mixed dentition vs the permanent dentition.
Methods
Fifty-four subjects were grouped as follows: 24 in the mixed dentition and 30 in the permanent dentition at the start of treatment. All patients had been treated with the Haas type of palatal expansion appliance followed by nonextraction fixed edgewise mechanics. Digitized dental casts were evaluated at 3 times: before treatment (T1), after treatment (T2), and at the long-term retention (T3). Intermolar widths were computed by subtracting measurements between time points, and comparisons between the groups were made to determine expansion and stability differences.
Results
Significant intermolar width increases were observed from T1 to T2 with significant relapses from T2 to T3, and an overall net gain remained at T3 in each group. No significant differences were found for relapse between the mixed and permanent dentitions.
Conclusions
There are no differences for the long-term intermolar width stability in patients treated with palatal expansion in the mixed dentition vs the permanent dentition.
Highlights
- •
Long-term intermolar width stability after palatal expansion was studied.
- •
Treatments in the mixed vs permanent dentition were compared.
- •
No significant differences were found in intermolar width stability.
- •
Absence or presence of crossbite did not affect stability.
Maxillary palatal expansion has been a widely used technique in orthodontics for decades, dating back to the 19th century when Angell and White first published on the technique in their pioneering work in The Dental Cosmos . After a period of rejection, the technique regained popularity in the literature in the 1900s and remains a widely used and accepted form of treatment in orthodontics. Palatal expansion is a proven and effective treatment to gain arch width and space as well as to eliminate crossbites and constriction. Although the immediate short-term dental and skeletal effects after palatal expansion are understood, inconsistency in the literature persists regarding treatment in the mixed vs the permanent dentitions and the associated stability. Advocates of early treatment with palatal expansion seek to eliminate crossbites early in an effort to help guide normal occlusal development. Additionally, in patients with severe early crowding, palatal expansion can assist in creating space to potentially avoid extractions during future orthodontic treatment and limit permanent tooth impactions. Contrary to advocates for early treatment, some clinicians support later treatment of palatal expansion in the permanent dentition, reporting that it leads to more stable results. Furthermore, if a posterior crossbite is not evident during the mixed dentition, the likelihood of one developing in the permanent dentition is low. Therefore, it may be more beneficial to use arch space maintenance until the permanent dentition is reached. Many studies have addressed the long-term stability of palatal expansion, but little attention has been focused on stability comparisons between the mixed and the permanent dentitions. Although there is no disagreement about treating a posterior crossbite early, stability is questioned. Furthermore, in the absence of a posterior crossbite, is there a difference in stability in patients treated in the mixed vs the permanent dentition? If no difference exists, it may be more advantageous to initiate palatal expansion in the permanent dentition barring any other warranted reasons. The purpose of this study was to determine the long-term intermolar width stability of palatal expansion performed in the mixed dentition vs the permanent dentition in patients who subsequently received fixed edgewise appliances.
Material and methods
A sample of 54 subjects was down-selected based on complete record availability from a group of 71 subjects from a collection of dental casts previously digitized with a scanner (R700; 3Shape, Copenhagen, Denmark) and stored at Saint Louis University’s Center for Advanced Dental Education. All records were collected from a private practice in which the same practitioner treated all patients. All received palatal expansion with the standard Haas type of appliance, which incorporates molar bands and, if present, bands on the first premolars with an acrylic pad against the palate in the jackscrew design. The expander remained in place for an average of 3 months once active expansion stopped. After expansion, all patients received nonextraction treatment with fixed edgewise appliances. After their treatment, a maxillary removable retainer and a mandibular bonded retainer from canine to canine were delivered and worn for approximately 6.5 years. The subjects were selected based on the following inclusion criteria.
- 1.
Maxillary and mandibular dental casts were available at 3 times: T1 (pretreatment), T2 (posttreatment), and T3 (long-term retention follow-up).
- 2.
The T1 records included either mixed dentition or permanent dentition, with the mixed dentition containing at least 2 deciduous teeth. Mixed dentition ranged from early to late mixed dentition.
- 3.
The maxillary permanent first molars were fully erupted.
The 54 adolescents were 18 or under at T1, with an average treatment time of 3.9 ± 2.3 years. The average length of the retention records was 11.0 ± 5.4 years. The sample was divided initially into 2 groups—mixed dentition and permanent dentition—based on the dentition stage at T1. The average treatment times for the mixed and permanent dentitions were 4.1 ± 2.3 and 3.8 ± 2.4 years, respectively. The average retention periods for the mixed and permanent dentitions were 10.5 ± 4.4 and 11.4 ± 6.2 years, respectively. The groups were further subdivided into 4 groups: mixed dentition crossbite, mixed dentition no crossbite, permanent dentition crossbite, and permanent dentition no crossbite at T1 ( Table I ).
| Group | Sample size (n) | Subgroup | Sample size (n) |
|---|---|---|---|
| Mixed dentition | 24 | Mixed, crossbite | 9 |
| Mixed, no crossbite | 15 | ||
| Permanent dentition | 30 | Permanent, crossbite | 15 |
| Permanent, no crossbite | 15 |
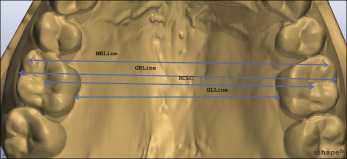
The previously digitized casts were analyzed using OrthoAnalyzer software (3Shape), which is accurate within 0.020 mm according to the manufacturer’s specifications. For each cast, 8 landmarks were selected to construct 4 lines between the maxillary first molars, which were used to calculate intermolar widths ( Figs 1 and 2 ). The landmark and line definitions are shown in Tables II and III , respectively.
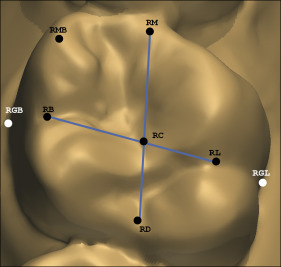
| Abbreviation | Landmark | Definition |
|---|---|---|
| RGB | Right gingival buccal | Intersection of buccal groove and gingival margin on maxillary right first molar |
| RGL | Right gingival lingual | Intersection of lingual groove and gingival margin on maxillary right first molar |
| RMB | Right mesiobuccal | Center of mesiobuccal cusp tip of maxillary right first molar |
| RM | Right mesial | Mesial marginal ridge midpoint on maxillary right first molar |
| RB | Right buccal | Point between buccal groove of maxillary right first molar on the occlusal surface |
| RD | Right distal | Distal marginal ridge midpoint on maxillary right first molar |
| RL | Right lingual | Point between lingual groove of maxillary right first molar on the occlusal surface |
| RC | Right center | Intersection of 2 lines drawn between RM/RD and RB/RL |
| LGB | Left gingival buccal | Intersection of buccal groove and gingival margin on maxillary left first molar |
| LGL | Left gingival lingual | Intersection of lingual groove and gingival margin on maxillary left first molar |
| LMB | Left mesiobuccal | Center of mesiobuccal cusp tip of maxillary left first molar |
| LM | Left mesial | Mesial marginal ridge midpoint on maxillary left first molar |
| LB | Left buccal | Point between the buccal groove of maxillary left first molar on the occlusal surface |
| LD | Left distal | Distal marginal ridge midpoint on maxillary left first molar |
| LL | Left lingual | Point between the lingual groove of maxillary left first molar on the occlusal surface |
| LC | Left center | Intersection of 2 lines drawn between LM/LD and LB/LL |
| Abbreviation | Line | Definition |
|---|---|---|
| MB line | Line from RMB to LMB | Line measuring distance between mesiobuccal cusp tips of maxillary first molars |
| GB line | Line from RGB to LGB | Line measuring distance between the gingival buccal margins of maxillary first molars |
| GL line | Line from RGL to LGL | Line measuring distance between the gingival lingual margins of maxillary first molars |
| RCLC | Line from RC to LC | Line measuring distance between the occlusal centers of maxillary first molars |
Lines were constructed between the gingival buccal margins (GB line), gingival lingual margins (GL line), constructed occlusal table center (RCLC), and mesiobuccal cusp tips (MB line). Using the tooth landmarks, the software calculated the intermolar widths between the maxillary first molars accurate to 0.01 mm. Linear measurements between each molar at each time point (T1, T2, and T3) were generated, and the data collected were for each patient.
Statistical analysis
We tested the null hypothesis, that there is no difference in the long-term intermolar width stability of palatal expansion treated in the mixed vs the permanent dentition. All measurements were taken from the digitized casts at T1, T2, and T3. The linear measurements obtained for each set of records were organized in Excel 2010 (Microsoft, Seattle, Wash). The amount of expansion from T1 to T2, the amount of relapse from T2 to T3, and the overall changes from T1 to T3 were calculated. Descriptive data collection and statistical analysis were performed using the Statistical Package for the Social Sciences (version 20; IBM, Armonk, NY) to compare the changes and associated statistics between the mixed and permanent dentition groups. Differences in each group were analyzed using paired t tests for each variable to compare changes during treatment for the mixed and permanent dentitions individually. Independent t tests were performed to determine whether there were significant differences between the 2 groups for the tested variables. One-way analysis of variance (ANOVA) in conjunction with the Tukey honestly significant difference tests were performed to compare stability differences between the subdivided groups: mixed dentition crossbite, mixed dentition no crossbite, permanent dentition crossbite, and permanent dentition no crossbite. A significance level of P <0.05 was set to assess the differences within and between the groups and subgroups.
Ten percent of the total sample was chosen at random to be reevaluated to assess the reliability of the measurements. Six patients were randomly chosen, and each intermolar width was remeasured at T1, T2, and T3. The Cronbach alpha was used to determine the reliability of the measurements. Reliability is considered acceptable if the intraclass correlations are greater than or equal to 0.80. The intraclass correlations for each variable and measurement were calculated, and all were found to be greater than 0.80. Therefore, the original measurements were deemed reliable.
Results
Descriptive statistics were performed for the mixed dentition and permanent dentition groups; the intermolar arch widths at T1, T2, and T3 for each variable are shown in Table IV .
| Variable | T1 | T2 | T3 | |||
|---|---|---|---|---|---|---|
| Mixed dentition | Permanent dentition | Mixed dentition | Permanent dentition | Mixed dentition | Permanent dentition | |
| RCLC | 42.29 ± 0.89 | 42.16 ± 0.80 | 48.46 ± 0.46 | 48.37 ± 0.45 | 47.97 ± 0.44 | 47.91 ± 0.42 |
| MB line | 45.03 ± 0.87 | 45.4 ± 0.88 | 52.35 ± 0.45 | 52.79 ± 0.52 | 51.64 ± 0.48 | 52.21 ± 0.50 |
| GL line | 31.00 ± 0.91 | 30.32 ± 0.74 | 36.83 ± 0.52 | 36.17 ± 0.42 | 36.41 ± 0.45 | 35.85 ± 0.38 |
| GB line | 50.35 ± 0.91 | 51.2 ± 0.77 | 57.30 ± 0.50 | 57.70 ± 0.50 | 56.58 ± 0.52 | 57.19 ± 0.49 |
Paired t test results for individual changes in the mixed and permanent dentition groups are given in Table V .
| Variable | T2 − T1 expansion | T3 − T2 relapse | T3 − T1 overall gains | |||
|---|---|---|---|---|---|---|
| Mean ± SD | Significance | Mean ± SD | Significance | Mean ± SD | Significance | |
| Mixed dentition | ||||||
| RCLC | 6.17 ± 3.49 | 0.002 ∗ | 0.49 ± 1.34 | 0.000 ∗ | 5.67 ± 3.48 | 0.002 ∗ |
| MB line | 7.33 ± 3.66 | 0.010 ∗ | 0.72 ± 1.49 | 0.000 ∗ | 6.61 ± 3.51 | 0.004 ∗ |
| GL line | 5.83 ± 3.37 | 0.000 ∗ | 0.41 ± 1.33 | 0.000 ∗ | 5.42 ± 3.33 | 0.000 ∗ |
| GB line | 6.95 ± 3.33 | 0.000 ∗ | 0.60 ± 1.32 | 0.000 ∗ | 6.35 ± 3.32 | 0.000 ∗ |
| Permanent dentition | ||||||
| RCLC | 6.21 ± 3.25 | 0.000 ∗ | 0.46 ± 0.98 | 0.016 ∗ | 5.75 ± 3.23 | 0.000 ∗ |
| MB line | 7.38 ± 3.81 | 0.000 ∗ | 0.59 ± 0.97 | 0.002 ∗ | 6.79 ± 3.74 | 0.000 ∗ |
| GL line | 5.85 ± 3.06 | 0.000 ∗ | 0.34 ± 1.00 | 0.074 | 5.51 ± 2.87 | 0.000 ∗ |
| GB line | 6.50 ± 3.01 | 0.000 ∗ | 0.52 ± 1.18 | 0.023 ∗ | 5.98 ± 2.96 | 0.000 ∗ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


