We successfully treated a Class II Division 2 patient with maxillary group distalization using interradicular miniscrews. A woman, aged 28 years 11 months, had a convex profile and an excessive overjet caused by a skeletal Class II jaw-base relationship. After leveling and alignment, titanium miniscrews were obliquely implanted between the maxillary second premolar and first molar. To distalize the maxillary dentition, nickel-titanium closing coil springs with a 2-N load were placed between the screws and the hooks on the archwire. After 28 months of active orthodontic treatment, a proper facial profile and an acceptable occlusion were achieved with a 4-mm distalization of the maxillary dentition. The resultant occlusion was stable throughout a 5-year retention period. Interradicular miniscrews were useful to distalize the maxillary dentition for correcting a Class II malocclusion. This new strategy, group distalization with miniscrews, can make the treatment simpler with greater predictability.
Highlights
- •
Maxillary group distalization of 4 mm can be achieved with interradicular miniscrews.
- •
The occlusion was stable after 5 years of retention despite the large amount of molar distalization.
- •
Extraction spaces of the mandibular first molars were completely closed with molar mesialization.
In the treatment of a Class II malocclusion, tooth extraction or nonextraction is a subject of much debate. In growing patients, growth modification is often tried to improve their anteroposterior jaw discrepancies without extractions. If a nongrowing patient has excessive overjet or a severe arch length discrepancy, orthodontists are likely to choose extraction treatment. However, most patients desire nonextraction treatment, if possible, and some do not accept extractions.
In such patients, orthodontists must seek other treatment options. Molar distalization can be an alternative to correct a Class II malocclusion. However, it is not easy to distalize the maxillary dentition completely with traditional orthodontic mechanics. Various types of molar distalizers have been developed and clinically used, but they cannot prevent counteractions: eg, flaring of the maxillary incisors. In addition, a group distalization of the maxillary dentition was almost impossible in most patients.
Recently, implant-anchored orthodontics has been shown to be effective in treating a wide variety of malocclusions. In particular, miniscrews have gained acceptance because they can provide stable anchorage for various types of tooth movement despite their small diameter and short length. Miniscrew anchorage can provide maxillary molar distalization without patient compliance and undesirable counteractions; therefore, now they are well regarded as a new treatment strategy for Class II correction. However, their long-term stability is still unknown.
In this case report, we demonstrate the 5-year retention of a group distalization of the maxillary dentition with interradicular miniscrews in an adult patient with a Class II Division 2 malocclusion.
Diagnosis and etiology
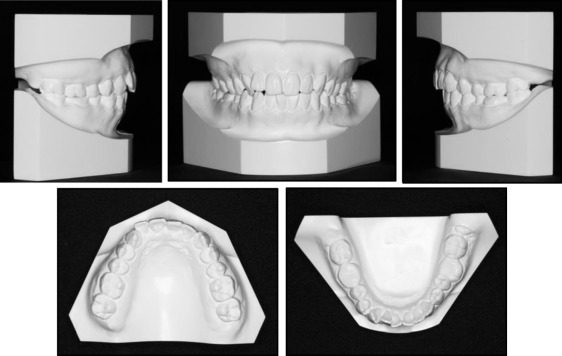
A woman, aged 28 years 11 months, had a chief complaint of esthetic problems of her maxillary incisors. Her facial profile was convex, and the frontal view was almost symmetric ( Fig 1 ). The molar relationships were Angle Class II on both sides ( Fig 2 ). Overjet and overbite were 5.0 and 0.0 mm, respectively. The maxillary and mandibular dental midline almost coincided with the facial midline. In the panoramic radiograph, the maxillary left central and right lateral incisors and the mandibular first molars were nonvital ( Fig 3 ). Periapical lesions were observed in the mandibular first molars. The maxillary third molars had already been extracted, but the mandibular third molars were impacted.

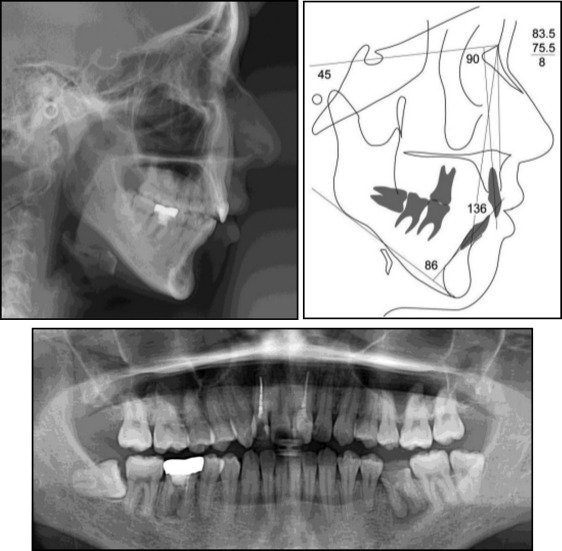
The cephalometric analysis, when compared with the Japanese norm, showed a skeletal Class II jaw-base relationship (ANB, 9.0°) ( Table ). The mandibular plane was steep (mandibular plane-SN, 44.0°). The maxillary incisors were lingually inclined (U1-SN, 90.0°), but the mandibular incisors showed an average inclination (L1-mandibular plane, 93.5°). As the result, the interincisal angle was increased (134.0°).
| Variable | Japanese norm ∗ | SD | Pretreatment | Posttreatment | Postretention |
|---|---|---|---|---|---|
| ANB (°) | 2.8 | 2.4 | 9.0 | 8.0 | 8.0 |
| SNA (°) | 80.8 | 3.6 | 85.0 | 84.0 | 84.0 |
| SNB (°) | 77.9 | 4.5 | 76.0 | 76.0 | 76.0 |
| Mandibular plane-SN (°) | 37.1 | 4.6 | 44.0 | 44.0 | 44.0 |
| U1-SN (°) | 105.9 | 8.8 | 90.0 | 88.5 | 88.5 |
| L1-mandibular plane (°) | 93.4 | 6.8 | 93.5 | 90.0 | 90.0 |
| Interincisal angle (°) | 123.6 | 10.6 | 134.0 | 137.0 | 137.0 |
| Overjet (mm) | 3.1 | 1.1 | 5.0 | 3.0 | 3.0 |
| Overbite (mm) | 3.3 | 1.9 | 0.0 | 3.0 | 3.0 |
Treatment objectives
The patient was diagnosed as having an Angle Class II Division 2 malocclusion with a skeletal Class II jaw-base relationship. An excessive overjet and a reduced overbite were also shown. The treatment objectives were to achieve (1) an acceptable occlusion with a good functional Class I occlusion and (2) an attractive smile and balanced facial profile.
To achieve a functional Class I occlusion, distalization of the maxillary dentition was necessary. Then, placement of interradicular miniscrews was planned in the posterior maxilla. The mandibular first molars would be extracted, and mesialization of the second and third molars was proposed to reduce the spaces for restorations.
Treatment objectives
The patient was diagnosed as having an Angle Class II Division 2 malocclusion with a skeletal Class II jaw-base relationship. An excessive overjet and a reduced overbite were also shown. The treatment objectives were to achieve (1) an acceptable occlusion with a good functional Class I occlusion and (2) an attractive smile and balanced facial profile.
To achieve a functional Class I occlusion, distalization of the maxillary dentition was necessary. Then, placement of interradicular miniscrews was planned in the posterior maxilla. The mandibular first molars would be extracted, and mesialization of the second and third molars was proposed to reduce the spaces for restorations.
Treatment alternatives
Several procedures were explored to achieve an acceptable occlusion. Extraction of the maxillary first premolars was considered to reduce the excessive overjet. However, the maxillary third molars had already been extracted, and 2 maxillary incisors were nonvital. Therefore, premolar extractions should be avoided to retain as many intact teeth as possible.
As for the mandibular first molars, prosthetic restorations without orthodontic treatment might shorten the total treatment period. However, this requires pulpectomy of the proximal teeth when bridge restorations are chosen. Moreover, dental implants are expensive and cause considerable surgical invasion, and their longevity is still unclear. Therefore, molar mesialization was planned to reduce the spaces for prosthetic restorations and to reconstruct the whole mandibular dentition with vital teeth.
Treatment progress
The mandibular first molars were extracted, and 0.022-in slot preadjusted edgewise appliances were placed on both arches. After leveling and alignment with nickel-titanium archwires, the mesialization of the mandibular second molars was started with closing-loop mechanics and a stainless steel archwire ( Fig 4 , A ).


