Introduction
The objectives of this study were to evaluate fixed bonded palatal surface retainers between the maxillary central incisors that were placed to maintain midline diastema closure and record their longevity, proclivity for damage, and periodontal health of the central incisors in patients 5 or more years after treatment.
Methods
Twenty-nine subjects were contacted and interviewed by phone concerning the status of their bonded retainer and midline diastema. Eleven subjects with intact retainers came for a periodontal health evaluation of the maxillary central incisors. The measures used were the plaque index, the periodontal screening and recording score, and the gingival index. A split-mouth design was used. Statistical analyses of retainer duration, damage probability, and gingival health were performed.
Results
Of the 29 subjects, 52% of the initial retainers were in place for an average of 23 years. For the total of 34 bonded retainers, the mean longevity was 17 years. The risk of breakage for any particular year the retainer was in place was 2%. The mean differences in scores between the maxillary central incisors and the control teeth were −0.06 for the plaque index, −0.14 for the periodontal screening and recording score, and −0.11 for the gingival index. Statistical tests on the differences indicated no evidence that the long-term presence of the bonded palatal surface retainer adversely affected the periodontal health of the maxillary central incisors.
Conclusions
The study’s sample demonstrated that a bonded retainer for maintaining closure of a maxillary midline diastema can last an average of 17 years or more, with a yearly 2% chance of breakage and with no expected adverse effects on the periodontal health of the maxillary central incisors.
Highlights
- •
Bonded retainers placed for retention of maxillary midline diastemas were evaluated.
- •
The sample comprised 29 subjects 8 to 33 years posttreatment.
- •
On average in this sample, the bonded retainers lasted for 17 years.
- •
There was a 2% chance for damage occurring to a retainer during any particular year.
- •
Long-term retainer use did not adversely affect the periodontal health of the central incisors.
Maxillary central incisors usually erupt with a space between them. As additional permanent teeth erupt by 16 years of age, 83% of the maxillary midline diastemas close. The reported incidences of maxillary midline diastema in adult dentitions range from 5% to 20%.
Patients with a maxillary midline disatema will often seek closure of the space, even though a recent study suggests that contemporary society may be more accepting of a midline diastema. Historically, orthodontists have experienced difficulty in retaining the closure of the space.
A number of etiologic factors have been implicated in the lack of physiologic closure of the maxillary midline diastema. Most factors could be classified as a genetic predilection. Generalized spacing because of the discrepancy between tooth size and available alveolar space is a possible factor. Problems with horizontal and vertical positions of the anterior teeth are another factor. Deleterious habits such as digital sucking and tongue position have also been mentioned. The most common factor associated with a retained maxillary midline diastema has been the labial frenum. Popovich et al found that low, thick frenum attachments were associated with 67% of the persistent maxillary midline diastemas.
Closure of the maxillary midline diastema can be achieved with several treatment modalities. Depending on the size and shape of the central incisors, prosthetic enlargement of the teeth to close the space could be an option. Also, removable or fixed orthodontic appliances can be used. The successful maintenance of diastema closure plays an important role in patient satisfaction, and clinicians have found that retaining the space closure can be a challenge.
Sullivan et al found that not much change occurred in the reopening of the maxillary spacing after 1 year of observation. Edwards found in a posttreatment study of maxillary midline diastema closure that 88% of the patients relapsed by 0.5 mm or greater. Edwards discussed the influence of the labial frenum and suggested a surgical procedure to reduce the tendency for relapse. The frenectomy protocol used by Edwards demonstrated beneficial results, even though it was not totally predictable. Removable retainers have always been used by orthodontists to retain changes in tooth position. The question is how long the patient needs to wear the removable retainer. The literature does not provide a definitive answer. Therefore, fixed retention that would physically prevent reopening of the space has been suggested.
If a clinician plans to use fixed retention between the maxillary central incisors, there are 2 questions: how long will the retainers last, and does long-term wear of the fixed retainer have any deleterious effects on the health of the maxillary central incisors. Studies have reported no evidence of hard or soft tissue lesions in relation to fixed bonded retainers for up to 3 years. Booth et al observed mandibular canine-to-canine bonded retainers in place for up to 20 years. They reported no detrimental effects on the periodontal health of the involved teeth using the gingival index to record periodontal health. A review of the literature showed no long-term evaluations of maxillary central incisor fixed retainers. Consequently, the objectives of this study were to observe the longevity of bonded palatal surface retainers between the maxillary central incisors, the proclivity for damage, and the periodontal health of the central incisors in patients at 5 or more years after treatment.
Material and methods
A list of all patients who received a fixed retainer for maintenance of a maxillary midline diastema closure was maintained by an author (A.H.M.). The first appliance was placed in 1981, and the same protocol was used for every patient and all retainers, and each was placed by the same operator. A stainless steel retainer (bonded lingual, central incisor to central incisor; TP Orthodontics, LaPorte, Ind) was bonded with a composite chemically cured bonding material (Concise orthodontic bonding system; 3M Unitek, Monrovia, Calif) to the palatal surfaces of the maxillary central incisors ( Fig 1 ). The criteria for placement were a pretreatment midline diastema of 1 mm or more and a posttreatment overbite that would accommodate placement without occlusal interference ( Fig 2 ).


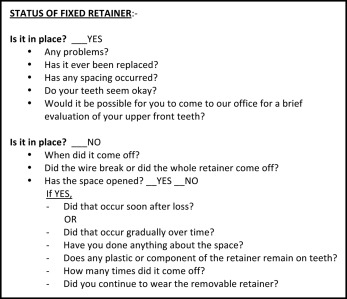
There were 102 consecutively treated patients who met the criteria and were a minimum of 5 years out of treatment. We attempted to contact all of them, and 30 were successfully contacted (29% contact rate). A phone interview was designed ( Fig 3 ) to determine the state of the fixed retainer and the maintenance of space closure for the maxillary midline diastema. If a retainer was damaged, details about the incidence were obtained. If the appliance was in place, we requested the patient to come for a clinical evaluation.
The clinical evaluation consisted of intraoral photographs of the retainers and the teeth in occlusion, and a periodontal evaluation. The periodontal evaluation consisted of recording the following 3 indexes in this order: (1) plaque index, a screening tool to assess plaque and debris deposition on the teeth; (2) periodontal screening and recording (PSR) score, a diagnostic screening tool for the early detection of periodontal disease measuring pocket depth; and (3) gingival index, a screening tool to evaluate the gingival status using bleeding points that appear after probing.
These indexes were measured for the maxillary central incisors and the control teeth in each sextant comprising the following teeth: maxillary arch—right first molar, right lateral incisor, and left first premolar; and mandibular arch—left first molar, left lateral incisor, and right first premolar. All measurements were made by 1 investigator (J.R.). This split-mouth design was used to compare each index evaluation of the maxillary central incisors with the average scores obtained from the control teeth as listed above.
Statistical analysis
Applicable statistical analyses were used for the data. The mean longevity was calculated for the overall sample and the groups based on the status of the retainer. The incidence rate for damage to the retainer was determined for the entire sample and for every 10-year period. The long-term periodontal health of the maxillary central incisors was measured by the 3 indexes and compared with the scores for the central incisors using statistical tests appropriate for the within-subject design of the study.
Results
To address the question of retainer longevity and potential damage to a retainer, 29 subjects (18 women, 11 men) were categorized into 4 groups according to the status of their palatally bonded retainer between the maxillary central incisors. Table I presents the summary statistics on retainer longevity for each group. Group 1, containing 15 subjects (51.7%), still had their first retainer in place at the time of the study. The average longevity for group 1 was 23.2 years, with a standard deviation (SD) of 4.8 years, a median of 22 years, and a range of 17 to 33 years. To make an inference on retainer longevity for the general population that the sample represented, the 95% confidence interval (CI) of the mean for group 1 was calculated to be between 20.6 and 25.8 years.
| Group | Subjects | Years with retainer | |||||
|---|---|---|---|---|---|---|---|
| (n) | % | Mean | SD | Median | Minimum | Maximum | |
| Group 1: First retainer | 15 | 51.7 | 23.2 | 4.8 | 22 | 17 | 33 |
| Group 2: Second retainer | 5 | 17.2 | 11.4 | 8.4 | 8 | 2 | 24 |
| Group 3: Retainer removed | 4 | 13.8 | 16.5 | 4.8 | 17 | 11 | 21 |
| Group 4: Retainer damaged | 5 | 17.2 | 10.8 | 5.3 | 8 | 6 | 17 |
| Total | 29 | ||||||
Group 2 contained 5 subjects (17.2%) who had a second retainer placed because of damage to the first retainer with an unacceptable reopening of the maxillary midline diastema. For those subjects, replacements occurred as follows: 1 was repaired after 2 years, 2 after 8 years, 1 after 15 years, and 1 after 24 years. On average, the first retainer in group 2 lasted 11.4 years (SD, 8.4 years). At the time of this study, the second replacement retainer was still in place; for these subjects, the retainers had lasted for 2, 3, 12, 16, and 20 years, respectively. This yielded an average of 10.6 years (SD, 7.9 years).
Groups 3 and 4 included a total 9 subjects who no longer had a retainer in place. The retainers for the 4 subjects in group 3 were removed by their general dentists, but they were still functioning at the time of removal. The average longevity for group 3 was 16.5 years (SD, 4.8 years). The 5 subjects in group 4 had experienced breakage of the first retainer. Their average longevity was 10.8 years (SD, 5.3 years). Subjects in both groups elected not to replace the bonded retainer because there was no significant space opening of the diastema.
Another way to analyze the sample and retainer longevity is to combine all retainers and examine their lifetimes. There were 29 original retainers plus 5 second retainers, for a total of 34 retainers in this sample. The mean longevity for these retainers was 17.0 years (SD, 8.1 years; median, 18 years). The 95% CI of the average longevity of all retainers was between 14.2 and 19.8 years.
Next, the incidence rate in which the possibility of something adverse happening to a retainer for any given year of its presence in the mouth was calculated for the total sample as well as for every 10-year period. Table II presents the results for the incidence rate calculations. Overall, there were 10 incidences in this sample: 5 from group 2 and 5 from group 4. Group 3 was not considered because the retainers were purposefully removed. Across all 29 subjects, the data consisted of 523 person-years at risk for a retainer failure (an incident). The incidence rate for the total sample was 0.019 per person-year; this is almost 2%. The 95% CI for the incidence rate was between 0.01 and 0.035.
| Person-year | Incidence (n) | Incidence rate | 95% CI | |
|---|---|---|---|---|
| All subjects | 525 | 10 | 0.019 | 0.01, 0.035 |
| By 10-year intervals | ||||
| 0-10 years | 269 | 6 | 0.022 | 0.01, 0.05 |
| 10-20 years | 195 | 3 | 0.015 | 0.005, 0.048 |
| 20-30 years | 58 | 1 | 0.017 | 0.002, 0.122 |
| >30 years | 3 | 0 | 0 |
The incidence rate was then calculated for the 10-year periods. Over time, the incidence rates were comparable between periods: the average rates were calculated to be 0.022 for the first 10 years, 0.015 for the next 10 years, and 0.017 between 20 and 30 years. The CIs for these rates overlap, suggesting that the incidence rates for less than 10 years, between 10 and 20 years, and between 20 and 30 years were not statistically different.
The long-term periodontal health of the maxillary central incisors was evaluated for 11 subjects at clinical examinations. Three measures of gingival health were used on each subject. A split-mouth design was used with the periodontal health of the maxillary central incisors (experimental) compared with the periodontal health of the rest of the mouth (control).
Table III presents summary statistics for the periodontal health measures that were used. The differences between the mean scores of the maxillary central incisors and the control teeth were the following.
- 1.
Plaque index: a mean difference of −0.06, with an SD of 0.10 and the 95% CI between −0.13 and 0.01.
- 2.
PSR score: a mean difference of −0.14, with an SD of 0.23 and the 95% CI between −0.29 and 0.02.
- 3.
Gingival index: a mean difference of −0.11, with an SD of 0.33 and the 95% CI between −0.34 and 0.11.
| n | Mean | SD | Median | Minimum | Maximum | |
|---|---|---|---|---|---|---|
| Plaque index | ||||||
| Affected area | 11 | 0.05 | 0.15 | 0 | 0 | 0.50 |
| Control | 11 | 0.11 | 0.14 | 0.08 | 0 | 0.42 |
| Difference | 11 | −0.06 | 0.10 | 0 | −0.25 | 0.08 |
| PSR | ||||||
| Affected area | 11 | 0 | 0 | 0 | 0 | 0 |
| Control | 11 | 0.14 | 0.23 | 0 | 0 | 0.67 |
| Difference | 11 | −0.14 | 0.23 | 0 | −0.67 | 0 |
| Gingival index | ||||||
| Affected area | 11 | 0.11 | 0.21 | 0 | 0 | 0.50 |
| Control | 11 | 0.23 | 0.26 | 0.17 | 0 | 0.83 |
| Difference | 11 | −0.11 | 0.33 | −0.17 | −0.83 | 0.50 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


