Introduction
One method of articulating digital models is to use a digitized interocclusal record. However, the accuracy of different interocclusal record materials to articulate digital models has yet to be evaluated.
Methods
A plastic typodont was modified with reference points for interarch measurements and articulated in maximum intercuspal position on a semiadjustable hinge articulator. Twenty-five interocclusal records of each of the 5 experimental materials (Regisil Rigid, Dentsply, York, Pa; Futar Scan, Kettenbach, Huntington Beach, Calif; Byte Right, Motion View Software, Chattanooga, Tenn; Aluwax, Aluwax Dental Products, Allendale, Mich; and Beauty Pink wax, Miltex, York, Pa) were made on the mounted typodont and digitized using an Ortho Insight 3D laser surface scanner (Motion View Software). Motion View Software was used to articulate the digital models by matching points from the models to the digitized interocclusal records. The distances between corresponding interarch markers were measured and compared with the measurements taken on the physical typodont (gold standard).
Results
Polyvinyl siloxane materials were significantly more likely to lead to successful articulation than were the other interocclusal record materials. Statistical analysis showed a significant effect of the bite registration material on the probability of success of the articulation ( P <0.005).
Conclusions
Polyvinyl siloxane is a more accurate interocclusal recording material when articulating digital models according to the process described in this study. Using a bite registration to articulate digital models should be considered the first step in the articulation process, with a likely residual need to manipulate the models manually.
Highlights
- •
Interocclusal records were made with 5 experimental materials and then digitized.
- •
Digital records were articulated, and a best-fit algorithm was used to align the models.
- •
Records made of polyvinyl siloxane performed best.
- •
No materials performed perfectly, and manual manipulation of the models is required.
Models provide information for diagnosis and treatment planning and function as a 3-dimensional (3D) record of the pretreatment malocclusion. Most treatment plans devised from study casts alone remain unchanged even with the addition of other diagnostic records such as photographs and radiographs. Study models and facial photographs are also keys to extraction decisions. The disadvantages of traditional plaster models include susceptibility to degradation, fracture, loss, space needed for storage, time required for retrieval, limited transferability, and limited diagnostic versatility. Digital models have numerous benefits over plaster models such as instant accessibility with no space required for storage and transferability for consulting with other clinicians. It is also possible to use digital models to create multiple diagnostic setups and save time when completing various measurements and analyses. Casts can also be split virtually to analyze the occlusion from the lingual aspect. A further benefit is the ability to integrate the detail from digital models onto cone-beam computed tomography scans to visualize tooth roots in a virtual setup or to plan orthognathic surgery. Digital models can also be used to superimpose pretreatment and posttreatment models to evaluate therapeutic outcomes.
Numerous studies have evaluated the accuracy and reliability of measurements made on digital models compared with plaster models and have determined that measurements on the 2 types of models are generally equivalent. Measurements on digital models have also been found to be more precise than those made on plaster models. Studies evaluating intra-arch measurements such as tooth size, arch length, and transverse measurements have shown that digital models are accurate and reliable. However, various interarch measurements such as molar classification, overjet, overbite, and occlusal contacts have shown some discrepancies. Interarch measurements are an essential part of diagnosis and treatment planning, and they depend on accurate articulation of the models.
Rheude et al evaluated how treatment plans devised using digital models changed after evaluating the original plaster models. Most treatment plans stayed the same, but the ones that changed were devised by using digital models that were incorrectly articulated. In addition, those authors found that diagnostic characteristics that changed between evaluations of digital and plaster models included several interarch characteristics including molar classification, canine classification, overbite, overjet, anterior and posterior crossbites, and midlines. All of these characteristics are contingent on accurate articulation of the models.
Accurately articulated digital models are important in orthognathic surgery planning. However, cone-beam computed tomography images do not provide enough surface detail of the teeth to be used to establish occlusion and fabricate surgical splints. Digital models provide accurate representations of occlusal surfaces and must be integrated into cone-beam computed tomography images for a complete and accurate representation. Digital models used for orthognathic planning and production of surgical splints have been shown to be successful except when there were errors in the digital mounting process that may be related to errors in the interocclusal recording process. If the interocclusal registration is not stable or accurate, it is impossible to achieve an accurate surgical splint.
When plaster models are articulated by hand, maximum intercuspation is established quickly and accurately with tactile feedback. In contrast, establishing maximum intercuspation with digital models is much more challenging. Without tactile feedback, models must be articulated visually. Many digital model-viewing programs, including the one used in this study, lack collision constraints, meaning that the separate 3D images of the maxillary and mandibular arches can continue to move through one another after contact is established. Digital models can be successfully aligned to produce contacts equivalent to those marked on plaster models. One method is to align the models manually using visual cues. However, visual alignment of digital models is time-consuming, frequently taking hours. Digital models can also be articulated by identifying paired contact points on opposing models, but identifying points can be inaccurate, especially in malocclusions. Chang et al, Chun et al, and Xia et al developed a 2-step method to articulate digital models, initially using a point-matching algorithm to align the maxillary and mandibular dental curves and then refining the occlusion using a surface-based minimum-distance mapping algorithm with collision constraints. Although their method has been validated, not all model-viewing softwares are programmed with this algorithm. Another method for articulating digital models is to scan the maxillary and mandibular plaster models in articulation to obtain an occlusion scan and use best-fit algorithms to align the models with the occlusion scan. Finally, the technique applied by the software in this study used a scanned image of an interocclusal record. Points on the models are identified and matched to points on the interocclusal record, and then a best-fit algorithm aligns the models to the registration. The advantage of using an interocclusal record is that it is easily made and provides an efficient guide for articulating the maxillary and mandibular models. Polyvinyl siloxane (PVS) interocclusal records have successfully been used to accurately articulate digital models. In contrast, wax interocclusal records have led to inaccurate representations of interarch relationships.
Several studies have evaluated which type of interocclusal record material most accurately articulates plaster casts, but no studies have evaluated which material is best for articulating digital models. The objectives of this study were to evaluate different types of interocclusal record material and to determine which material is optimized for laser scanning, and which most accurately articulates digital models.
Material and methods
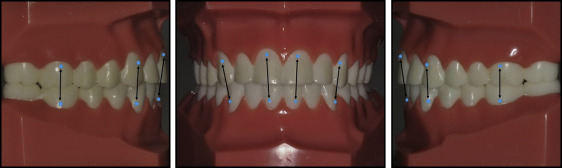
A plastic typodont (005-000; American Orthodontics, Sheboygan, Wis) was modified using a US No. 1/2 round bur to make semicircular indentations at 12 points near the gingival margins of the maxillary and mandibular first molars, canines, and central incisors. The locations are shown in Figure 1 . The typodont was then digitized using an Ortho Insight 3D laser surface scanner (Motion View Software, Chattanooga, Tenn). The digital models were inspected to ensure that indentations were captured during the scanning process. The typodont was then mounted in a semiadjustable articulator (Panadent, Colton, Calif) in maximum intercuspal position. The distance between corresponding interarch markers was measured using digital calipers (ProDent USA, New Brunswick, NJ). The measurements were repeated 10 times, and the mean distance for each of the 6 measurements was used as the gold standard.
Five interocclusal record materials were tested in this study: Regisil Rigid PVS (Dentsply, York, Pa), Futar Scan PVS optimized for optical scanning (Kettenbach, Huntington Beach, Calif), Byte Right thermoplastic bite registration material (Motion View Software, Chattanooga, Tenn), Aluwax aluminum-based wax (Aluwax Dental Products, Allendale, MI), and Beauty Pink hydrocarbon wax (Miltex, York, Pa). Twenty-five interocclusal records of each of the 5 experimental materials were made on the typodont in maximum intercuspal position. The PVS materials were expressed onto the occlusal surfaces of the mandibular teeth, and the articulator was closed with manual pressure until the teeth were contacting in maximum intercuspation. A 500-g weight was placed on top of the articulator while the material set to prevent any expansion during setting from changing the occlusion. The thermoplastic and wax materials were heated in a water bath according to the manufacturers’ instructions (Byte Right, 77°C; Aluwax, 40°C; Beauty Pink wax, 50°C). The materials were then placed on the occlusal surfaces of the mandibular teeth, and the articulator was closed until the teeth were contacting in maximum intercuspation. A 500-g weight was placed on top of the articulator while the material cooled and hardened. Each bite registration was digitized using the Ortho Insight 3D laser surface scanner and the Motion View software within 10 minutes of setting. The digitized bite registrations were then used to articulate the maxillary and mandibular digital models using the software to identify the teeth on both the models and the bite registrations. A best-fit surface-matching algorithm fits the maxillary model to the upper surface of the bite registration and the mandibular model to the lower surface. The occlusion resulting from this process was not modified, and the distance between corresponding interarch markers was measured using Motion View software’s linear distance measuring tool.
Statistical analysis
All statistical analyses were performed with Stata software (StataCorp, College Station, Tex). For each interarch measurement, analysis was performed using a linear regression model with dummy variable coding for impression material and robust Huber-White sandwich estimator of the variance to account for the inequality of the variances between materials. To quantify the overall accuracy of the articulation, a “successful articulation” was defined as a result in which all 6 interarch measurements were within 0.5 mm of the gold standard. The limit of 0.5 mm was chosen based on clinical relevance and the American Board of Orthodontics’ increments for grading plaster models. A logistic regression model was used to predict the probability of a successful articulation based on the material used. The Wald chi-square test of the logistic regression model was used to determine the significance of the effect of the interocclusal record material on the probability of the success of the articulation.
Results
Most interarch measurements differed significantly from the gold standard measurements regardless of the material used to articulate the digital models ( Table I ). The Wald chi-square test of the logistic regression model showed a significant effect of the bite registration material on the probability of success of the articulation ( P <0.005). Regisil Rigid had higher odds for successful articulation than Byte Right (odds ratio [OR], 0.30; 95% confidence interval [CI], 0.09-1.00), Aluwax (OR, 0.12; 95% CI, 0.03-0.44), and Beauty Pink wax (OR, 0.10; 95% CI, 0.03-0.36) ( Table II ). The difference in odds of successful articulation between Regisil Rigid and Futar Scan (OR, 0.42; 95% CI, 0.13-1.37) was not statistically significant.
| Material | Right molar coefficient (95% CI) | Right canine coefficient (95% CI) | Right central incisor coefficient (95% CI) | Left central incisor coefficient (95% CI) | Left canine coefficient (95% CI) | Left molar coefficient (95% CI) |
|---|---|---|---|---|---|---|
| Regisil Rigid | 0.43 (0.36-0.50) ∗ | 0.07 (−0.03 to 0.17) | 0.11 (0.00-0.22) ∗ | −0.04 (−0.13 to 0.05) | 0.07 (−0.03 to 0.17) | 0.30 (0.23-0.37) ∗ |
| Futar Scan | 0.43 (0.36-0.51) ∗ | 0.14 (0.04-0.24) ∗ | 0.24 (0.14-0.34) ∗ | 0.05 (−0.04 to 0.15) | 0.21 (0.11-0.31) ∗ | 0.41 (0.22-0.48) ∗ |
| Byte Right | 0.34 (0.18-0.50) ∗ | 0.17 (−0.04 to 0.38) | 0.34 (0.09-0.59) ∗ | 0.18 (−0.06 to 0.43) | 0.33 (0.11-0.56) ∗ | 0.50 (0.37-0.63) ∗ |
| Aluwax | 0.56 (0.45-0.66) ∗ | 0.27 (0.09-0.45) ∗ | 0.42 (0.21-0.64) ∗ | 0.27 (0.05-0.49) ∗ | 0.42 (0.21-0.62) ∗ | 0.68 (0.53-0.83) ∗ |
| Beauty Pink wax | 0.56 (0.19-0.94) ∗ | 0.75 (0.50-1.00) ∗ | 0.95 (0.75-1.14) ∗ | 0.73 (0.54-0.93) ∗ | 0.58 (0.33-0.83) ∗ | 0.06 (−0.22 to 0.33) |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


