Introduction
The aim of this study was to compare the prevalence of agenesis of the maxillary lateral incisors in the cleft area of patients with unilateral cleft lip and palate with and without Simonart’s band.
Methods
A sample of panoramic radiographs of 121 patients with a mean age of 7 years was divided into 2 groups: group 1 included 60 patients with Simonart’s band, and group 2 included 61 patients without Simonart’s band. Patients with syndromes were not included. Chi-square tests were used for intergroup comparisons ( P <0.05).
Results
In the pooled subgroup, the prevalences of maxillary lateral incisor agenesis, supernumerary maxillary lateral incisors, 1 maxillary lateral incisor mesial to the cleft, and 1 maxillary lateral incisor distal to the cleft were 40.5%, 12.5%, 8.2%, and 38.8%, respectively. In group 1, these frequencies were 35%, 10%, 6.7%, and 48.3%; in group 2, they were 45.9%, 13.1%, 11.5%, and 29.5%. There was a statistically significant difference between the groups for the prevalence of a maxillary lateral incisor distal to the cleft.
Conclusions
The presence of Simonart’s band is associated with a higher frequency of maxillary lateral incisor development in the maxillary process.
It has been proposed that clefting is part of a complex malformation associated with other dental anomalies. According to Hoffmeister’s genetic study, some microsymptoms such as hypodontia, hyperodontia, fusion of teeth, and twin formation have a common genetic background. Since the cleft is located at the border of the primary and secondary palates, dental anomalies in this area are common.
Previous embryologic studies have demonstrated that the maxilla is derived from the maxillary process, which originates from the first pharyngeal arch, called the maxillary growth center, and the premaxilla, which originates from the frontonasal prominence and part of the lateral nasal prominence. During prenatal development, the medial part of the maxillary process delivers material to the future premaxilla. Therefore, after ossification, the incisive suture delimitating the posterior and anterior segments of the maxilla is positioned more mesially than is the fusion site between the premaxilla and the maxillary processes.
In 3-dimensional reconstructions, it was possible to observe 2 thickenings of the dental epithelium originating independently from the medial nasal and maxillary processes separated by a narrow groove. The fusion site of the dental epithelia was detectable as a furrow on the germ of the lateral incisor. Therefore, the mesial half of the maxillary lateral incisor might derive from the premaxilla, and the distal half of maxillary lateral incisor might derive from the maxillary process.
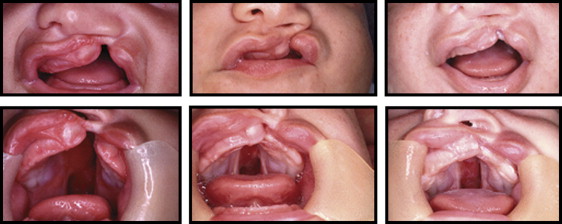
This presumed double origin of the lateral incisor could explain the high frequency of dental anomalies of number observed in patients with cleft lip and palate. Those with complete unilateral cleft lip and palate might have agenesis of the maxillary lateral incisors in the cleft region, supernumerary maxillary lateral incisors (1 mesial and 1 distal to the cleft region), or only 1 maxillary lateral incisor that might be positioned mesially or distally to the cleft. The prevalence of these anomalies might be associated with the degree of hypoplasia of the facial processes. In patients with unilateral cleft lip and palate, it is common to observe a tissue known as Simonart’s band ( Fig 1 ). This band is a tissue originating from a supplementary growth center of the maxillary process, called maxillary prime, which grows to form a bridge between the premaxilla and the lateral nasal prominence. The prevalence of Simonart’s band in patients with unilateral cleft lip and palate is approximately 20%. The presence of this band might mean fewer hypoplastic embryologic processes. Hence, a smaller prevalence of agenesis of maxillary lateral incisors distal to the cleft can be expected in patients with Simonart’s band. However, no previous studies have investigated these associations. The aim of this study was to verify the prevalence of maxillary lateral incisor agenesis at the cleft area in patients with unilateral complete cleft lip and palate, comparing patients with and without Simonart’s band. The null hypothesis tested in this study was that those with and without Simonart’s band have the same prevalence of dental anomalies related to maxillary lateral incisors at the cleft area.
Material and methods
From an initial sample of 275 patients with unilateral complete cleft lip and palate (born between 1989 and 1992) from the files of the Hospital of Rehabilitation of Craniofacial Anomalies, University of São Paulo in Brazil, all patients with Simonart’s band (n = 61) were selected. A control group of 61 patients without Simonart’s band was randomly selected from the same initial sample, matched by age and sex according to chi-square tests. One patient was excluded from the experimental group because of an incomplete set of intraoral photographs. Therefore, the sample included 121 patients with unilateral cleft lip and palate in the mixed dentition (36 girls, 85 boys) with ages ranging from 5 to 9 years. The radiographs were taken before the prebone graft orthodontic treatment. The exclusion criterion was patients with syndromes. Facial and intraoral photographs were analyzed to verify the presence of Simonart’s band. The sample was divided into 2 groups: group 1 comprised 60 patients with Simonart’s band with a mean age of 7 years and a male:female ratio of 3:1, and group 2 comprised 61 patients without Simonart’s band with a mean age of 7 years and a male:female ratio of 2:1.
Using panoramic and periapical radiographs, the maxillary lateral incisor in the cleft area was classified into 4 categories based on the distribution pattern of the cleft side according to the methodology established by Dentino et al : subgroup M, subjects with 1 tooth located on the mesial side of the alveolar cleft; subgroup D, subjects with 1 tooth located on the distal side of the alveolar cleft; subgroup MD, subjects with 2 teeth, 1 mesial and 1 distal to the cleft; and subgroup ABS, subjects with congenital absence of teeth in the cleft area ( Fig 2 ).

The prevalence of these 4 situations was calculated for both groups and for subgroups M, D, and MD pooled. The chi-square test was used for the intergroup comparison ( P <0.05). Based on the desired sample comparison in the study, and at an alpha value of 0.05, a sample size of 60 subjects for each group was found to provide a power of 0.70.
Results
The Table shows the intergroup comparison for the prevalences in subgroups M, D, MD, and ABS. The patients with Simonart’s band demonstrated a higher prevalence of 1 maxillary lateral incisor located on the distal side of the alveolar cleft, compared with the patients without Simonart’s band.
| Group | Group 1 (with band) | Group 2 (without band) | P | Pooled subgroups | |||
|---|---|---|---|---|---|---|---|
| Position | n | % | n | % | n | % | |
| Subgroup M | 4 | 6.7 | 7 | 11.5 | 0.36 | 72 | 59.5 |
| Subgroup D | 29 | 48.3 | 18 | 29.5 | 0.03 ∗ | ||
| Subgroup MD | 6 | 10 | 8 | 13.1 | 0.59 | ||
| Subgroup ABS | 21 | 35 | 28 | 45.9 | 0.22 | 49 | 40.50 |
| Subtotal | 60 | 100 | 61 | 100 | 121 | 100 | |
Results
The Table shows the intergroup comparison for the prevalences in subgroups M, D, MD, and ABS. The patients with Simonart’s band demonstrated a higher prevalence of 1 maxillary lateral incisor located on the distal side of the alveolar cleft, compared with the patients without Simonart’s band.


