Introduction
The aims of this study were to evaluate condylar and ramal mandibular vertical asymmetry in a patient group affected by unilateral (UCLP) and bilateral (BCLP) cleft lip and palate, and to compare the findings with a well-matched control group with normal occlusion.
Methods
The study groups included 20 UCLP patients (12 male, 8 female), 21 BCLP patients (12 male, 9 female), and a control group of 21 subjects with normal occlusion (10 male, 11 female). Measurements of condylar, ramal, and condylar plus ramal heights and asymmetry indexes were examined on cone-beam computed tomography images. One-way analysis of variance was used to determine potential statistical differences among the groups for condylar, ramal, and condylar plus ramal asymmetry index measurements. The post-hoc Tukey HSD test was used to determine individual differences.
Results
No investigated group showed a statistically significant sex difference for any asymmetry index ( P >0.05). There was a statistically significant difference between the normal and cleft sides in the ramal height and ramal plus condylar height measurements in the UCLP group ( P = 0.004 and P = 0.006, respectively). The Tukey HSD test showed a statistically significant difference between the UCLP and BCLP groups in terms of ramal asymmetry index values ( P = 0.018).
Conclusions
The ramal height and ramal plus condylar height measurements were significantly lower in the cleft side in the UCLP patients, and there was a statistically significant difference in ramal asymmetry index values between the patients affected by UCLP and BCLP.
Patients affected by cleft lip and palate (CLP) exhibit different growth patterns of the dentomaxillofacial tissues than do their normal peers and commonly have anterior and posterior crossbite tendencies caused by scarring. The crossbite side, especially unilateral posterior crossbite, is related to asymmetrical muscular function. Prolongation of abnormal muscular functions can cause changes in the growth center at the temporomandibular joint because the condyle is one of the most sensitive areas to occlusal changes.
Some studies have reported mandibular asymmetry in patients affected by CLP, whereas others, through the use of different radiographs and assessment techniques, have claimed that patients affected by CLP have no asymmetric mandible. For the first time reported in the literature, Habets et al applied a method to assess vertical mandibular asymmetry. This new method, which compares the vertical height of the right and left condyles and rami, has been used by some researchers to compare condylar asymmetry in unilateral and bilateral posterior crossbite patients, patients with temporomandibular disorders, early bilateral first molar extraction patients, and patients with Class II and Class III malocclusions. Recently, Kurt et al found no statistically significant differences among unilateral (UCLP) and bilateral (BCLP) cleft lip and palate groups and a control group with normal occlusion, using the method of Habets et al.
All of these mentioned studies on vertical mandibular asymmetry were performed with panoramic radiographs, which enable scanning of end-to-end structures of the entire dental system with relatively limited radiation doses and reduced financial costs to patients and health service providers. Nevertheless, there are some disadvantages to panoramic radiographs, such as inconstant magnification, image distortion, and vertical measurements that might be affected by the patient’s head position. However, cone-beam computed tomography (CBCT) technology makes it feasible to achieve true (1:1 size) images without magnification and with a relatively lower radiation dose and lower cost than with computed tomography.
Although studies on vertical condylar asymmetry have increased in recent years, to date, no study has been done with CBCT images to investigate condylar asymmetry in groups of UCLP and BCLP patients and compare them with a normal occlusion sample. Therefore, in this study, we aimed to determine whether there is an increase in condylar asymmetry associated with patients affected by UCLP and BCLP compared with an unaffected control population, using CBCT images according to the method described by Habets et al.
Material and methods
This study was carried out on the CBCT radiographs selected from the archives of the Departments of Oral and Maxillofacial Radiology and Orthodontics of the Faculty of Dentistry, Erciyes University, Kayseri, Turkey. The CBCT scans of the patients included in this study were part of the diagnostic records collected for patients with impacted teeth or those who required orthodontic treatment; the patients were not exposed to any additional radiation. Therefore, approval from the ethics committee was not required for this retrospective archive study. In addition, as a usual protocol, all patients (or parents) signed an informed consent agreeing to the use of the patients’ data for scientific studies.
The patients were divided into 3 groups: (1) 20 patients (12 male, 8 female) affected by UCLP, (2) 21 patients (12 male, 9 female) affected by BCLP, and (3) 21 patients (10 male, 11 female) as the control group. Subjects in the control group with normal occlusion met the following criteria, as suggested by Kurt et al : (1) Class I canine and molar relationships with minor crowding, normal growth, and normal development, including normal skeletal relationship and facial balance; (2) all teeth present except third molars; (3) no history of trauma, previous orthodontic or prosthodontic treatment, or maxillofacial surgery; and (4) no significant medical history.
All images were obtained with the patient in the supine position using CBCT (NewTom 5G; QR srl, Verona, Italy). Scanning time was 18 seconds, collimation height was 13 cm, exposure time was 3.6 seconds, and voxel size was 0.3 mm 3 . Digital Imaging and Communications in Medicine (DICOM) files obtained from the CBCT scans were reconstructed using NNT viewer software (QR S.r.l., Verona, Italy). All measurements were made by 1 author (S.K.B.). In addition, the cervical vertebra maturation stages of all patients were determined according to the method of Hassel and Farman.
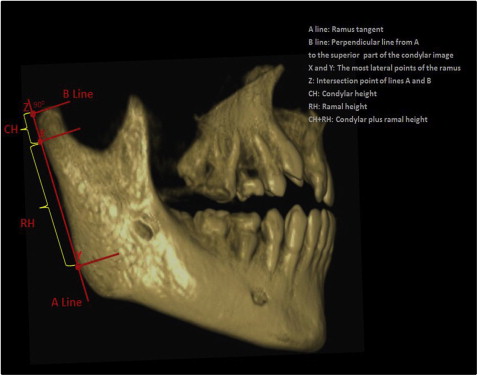
On both sides, the most posterior points of the condyle and ramus of the mandible were marked as the X and Y points. A line was drawn through X and Y and called the A-line. Another line, called the B-line, was drawn from the most superior points of the condyle perpendicular to the A-line. The confluence of the A-line and B-line was called point Z. The distance between points X and Z was measured as condylar height. In addition to this measurement, the distance between X and Y and the distance between Z and Y were measured as ramus height and condylar plus ramus height, respectively ( Fig ).
Finally, the vertical mandibular asymmetry indexes of the condyle, ramus, and condyle plus ramus were calculated using the following formula, developed by Habets et al : Asymmetry index (%): [(Right − Left)/ (Right + Left)] × 100
Statistical analysis
Two weeks after the first measurements, 20 randomly selected CBCT images were retraced and remeasured by the same author. The method error coefficient was calculated with Dahlberg’s formula. Dahlberg’s method error values were within acceptable limits (range, 0.409-0.954). In addition, the difference between the 2 tracings was tested for significance with a paired t test; no significant difference was found ( P >0.05), confirming the intraobserver reliability of the measurements.
Data regarding the asymmetry measurements were computed. The normality test of the Shapiro-Wilks and the Levene variance homogeneity test were applied to the data; all data were found to be normally distributed. Thus, the comparisons among the groups and sexes were analyzed using parametric tests. The Student t test was used to compare the sexes, and 1-way analysis of variance (ANOVA) was used to compare the asymmetry indexes among the UCLP, BCLP, and control groups. The Tukey HSD post-hoc test was performed to determine individual differences. In addition, a paired t test was used to determine possible statistical differences between the sides for condylar height, ramal height, and condylar height plus ramal height measurements in all groups.
All statistical analyses were performed with SPSS software (version 15.0 for Windows; SPSS, Chicago, Ill); P <0.05 was considered statistically significant.
Results
Table I shows descriptive data of the patients in the study. Sex distribution and chronologic ages in all groups were well matched (tested by chi-square and 1-way ANOVA, respectively; P >0.05 for both tests). The chronologic ages of the patients affected by UCLP and BCLP and the normal occlusion controls were 14.26 ± 3.88, 14.49 ± 2.47, and 14.29 ± 2.23 years, respectively.
| Group | Sex | Age (y) | Number | Sex comparison | UCB | BCB | Cervical vertebral maturation (CVM) stage | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | |||||||
| UCLP | Male | 15.49 ± 3.84 | 12 | NS | 3 | 2 | 2 | 3 | 2 | 1 | 2 | 2 |
| Female | 12.42 ± 3.36 | 8 | 2 | 1 | 4 | 0 | 3 | 0 | 0 | 1 | ||
| Total | 14.26 ± 3.88 | 20 | 5 | 3 | 6 | 3 | 5 | 1 | 2 | 3 | ||
| BCLP | Male | 14.38 ± 2.48 | 12 | NS | 4 | 6 | 3 | 2 | 2 | 3 | 1 | 1 |
| Female | 14.63 ± 2.59 | 9 | 3 | 4 | 0 | 1 | 1 | 1 | 2 | 4 | ||
| Total | 14.49 ± 2.47 | 21 | 7 | 10 | 3 | 3 | 3 | 4 | 3 | 5 | ||
| Normal occlusion | Male | 13.85 ± 2.22 | 10 | NS | 0 | 0 | 0 | 2 | 1 | 4 | 3 | 0 |
| Female | 14.69 ± 2.26 | 11 | 0 | 0 | 0 | 1 | 2 | 4 | 2 | 2 | ||
| Total | 14.29 ± 2.23 | 21 | 0 | 0 | 0 | 3 | 3 | 8 | 5 | 2 | ||
| Group comparison | NS | NS | ||||||||||
The descriptive mandibular asymmetry indexes for both sexes were calculated separately in the normal occlusion and CLP patient groups to investigate the relationship between the sexes. Because no statistically significant differences were found for these mean values, the data were pooled for further analyses ( Table II ).
| Group | Variable (%) | Male ( n = 34) | Female ( n = 28) | P | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| UCLP ( n = 20) (F/M, 8/12) | CAI | 10.87 | 8.89 | 11.59 | 7.57 | 0.851 |
| RAI | 4.30 | 5.73 | 3.72 | 2.29 | 0.791 | |
| CRAI | 3.83 | 5.50 | 2.90 | 1.70 | 0.649 | |
| BCLP ( n = 21) (F/M, 9/12) | CAI | 8.81 | 8.36 | 6.88 | 7.95 | 0.598 |
| RAI | 1.53 | 1.85 | 1.49 | 1.89 | 0.954 | |
| CRAI | 1.47 | 1.57 | 1.63 | 1.81 | 0.827 | |
| Normal occlusion ( n = 21) (F/M, 11/10) | CAI | 11.00 | 11.68 | 13.12 | 7.76 | 0.627 |
| RAI | 2.50 | 1.21 | 2.48 | 1.16 | 0.970 | |
| CRAI | 1.98 | 1.75 | 2.19 | 1.64 | 0.788 | |
Means, standard deviations, and statistical results of paired t tests comparing the condylar height, ramal height, and condylar height plus ramal height measurements of the normal and cleft sides in the UCLP group, and the left and right sides in the BCLP and the normal occlusion groups are shown in Table III . There were no statistically significant differences in the condylar height, ramal height, and condylar height plus ramal height measurements between the right and left sides in the BCLP and control groups; however, there were statistically significant differences in ramal height and condylar height plus ramal height measurements between the normal and cleft sides in the UCLP groups ( P = 0.004 and P = 0.006, respectively). The ramal height values were 42.70 ± 5.63 mm in the normal side and 40.24 ± 6.76 mm in the cleft side; the condylar height plus ramal height values were 46.11 ± 6.01 mm in the normal side and 43.80 ± 7.19 mm in the cleft side.
| Variable | UCLP | BCLP | Normal occlusion | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Normal side | Cleft side | P | Right side | Left side | P | Right side | Left side | P | |
| Mean (mm) | Mean (mm) | Mean (mm) | Mean (mm) | Mean (mm) | Mean (mm) | ||||
| CH | 3.41 ± 0.95 | 3.56 ± 0.84 | 0.489 | 3.41 ± 0.72 | 3.66 ± 0.81 | 0.148 | 4.41 ± 0.89 | 4.01 ± 0.83 | 0.156 |
| RH | 42.70 ± 5.63 | 40.24 ± 6.76 | 0.004 | 39.34 ± 3.79 | 39.42 ± 3.41 | 0.839 | 42.67 ± 4.76 | 42.07 ± 5.26 | 0.252 |
| CH + RH | 46.11 ± 6.01 | 43.80 ± 7.19 | 0.006 | 42.75 ± 3.99 | 43.08 ± 3.98 | 0.442 | 47.08 ± 5.11 | 46.08 ± 5.54 | 0.054 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


