(1)
Department of Endodontics, Nova Southeastern University College of Dental Medicine, Fort Lauderdale, FL, USA
The success of nonsurgical endodontic root canal treatment requires the use of files and instruments to remove necrotic and infected tissues. The steps in this process are to use a hand file to obtain patency in all the root canals of a tooth, to measure the working length of the teeth, and then to use rotary instruments to shape the root canals in preparation for their sealing and obturation. If these steps are performed correctly, endodontic treatment can retain a tooth that would otherwise require extraction.
Cleaning and Shaping of the Root Canals
Cleaning and shaping are separate concepts but are always performed together [1]. The goal of cleaning the root canal is the removal of necrotic pulp and infected tissues. The goal of shaping the canal is to maintain the apical foramen as small as possible in its original anatomical position [2]. A good endodontic treatment outcome is dependent on the removal of necrotic pulp and infected tissues to a low level that cannot cause a flare-up which will require retreatment. If the root canals are cleaned and shared adequately, the flare-up rate can be less than 2 % of cases [3], although there are some reports of a 10 % flare-up rate [4]. Teeth with a less infected root canal, or which have been infected with microorganisms for less time, generally lack a periradicular pathosis, and the success of endodontic treatment in these teeth is generally higher [5]. Teeth which have a periradicular pathosis on radiographs are more infected, and these teeth are more difficult to treat [6] and have a higher risk of flare-ups and requiring retreatment. The most significant factors affecting the instrumentation of teeth are tooth anatomy and morphology and the types of instruments and irrigants used for treatment [7]. Instruments must contact the root canal tissues to debride the canal; however, it has been shown that most of the root canal surfaces are not touched by hand files or instruments, even with the best efforts of the dentists [8]. The reasons why most of the surfaces are not touched are because of the ribbon, conical, or irregular shape of the canal, in addition to the presence of accessory canals, lateral canals, canal curvatures, fins, cul-de-sacs, and isthmuses which make total debridement virtually impossible (Fig. 6.1) [9].
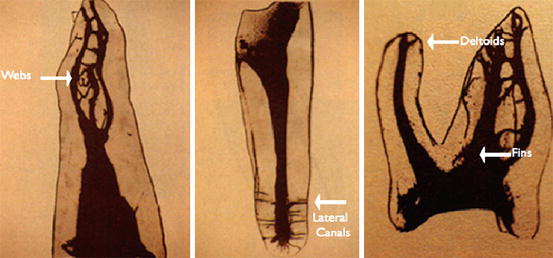
Fig. 6.1
Problems for cleaning and shaping root canals
Because of these obstacles in accomplishing the complete debridement and total elimination of infection inside the root canal, the goal of cleaning and shaping is to maximize the removal of necrotic and infected tissues [3], thereby reducing the risk of a flare-up and failure of the treatment. Prior to beginning root canal treatment, the case should take into account all these factors for its degree of difficulty; if it is beyond the experience and skills of the dentist, it should be referred to a specialist for supervision or treatment.
Root Canal Instrumentation
After a straight-line access, cavity has been cut to allow direct access of the instruments into the root canals, and the orifices of the root canals have been identified. The next step is to instrument the root canals. The instrumentation process can be simplified by dividing the procedure in a series of steps. The majority of teeth are approximately 19–25 mm in length. Most roots are 9–15 mm, and most crowns are 10 mm in length [10]. An easy concept is to divide the root canal into three regions: coronal, middle, and apical. Each of these regions is likely to be between 3 and 5 mm in length [10]. Dividing the root canal into three regions is a helpful strategy for instrumenting complicated calcified root canals with a challenging morphology.
Most guidelines for endodontic associations recommend that the root canal is irrigated with undiluted sodium hypochlorite (NaOCl) [11] at concentrations of 5.25, 6.1, and 8 %; however, many dentists dilute the concentration of NaOCl by half to 3 %, or even more to 1.5 % [12]. The main reasons for diluting the NaOCl are to limit the injury caused to a patient if the NaOCl spills or leaks [13].
After checking the preoperative radiographs of the tooth to be treated, the 0.02 tapered 10 and 15 stainless steel hand files are measured and curved by the dentist to match the length and curvature of the root canal [14]. These hand files are then placed inside the tooth to explore the coronal and middle thirds of the root canals. When the hand files are placed inside the canal and have been rotated to remove the tissue and make some space, a syringe is used to deliver a small volume of NaOCl into the space. The NaOCl can help lubricate the file and reduce the friction of the movement of the hand files into the canals. Once the hand files have progressed through the coronal and middle regions of the root canals, the canal maybe enlarged using the hand files prior to instrumentation with rotary NiTi root canal shaping instruments. After the coronal and middle thirds of the root canal are negotiated, small hand files are used to scout the remaining apical third of the canal [10, 15]. After this stage in the instrumentation of the root canal, it must be measured to avoid over-instrumentation.
Tooth Length Measurement
It is necessary to accurately measure tooth length in order to carry out and fulfill the basic tenets of root canal therapy [16]. This measurement should be 0.5–1-mm short of the radiographic apical foramen to create an apical stop within the tooth structure in order to confine instrumentation and the filling material [10, 15]. A goal in root canal treatment is to reduce intraradicular microorganisms to a level below that necessary to induce or sustain apical periodontitis [17]. Prior to instrumentation, it is essential to accurately measure the tooth working length during root canal preparation to avoid the accidental extrusion of irrigating solution and dressing or filling material, which can lead to persistent periapical inflammation and postoperative pain [18, 19]. The accuracy of the working length can have an impact on the outcomes of endodontic treatments [20, 21], and optimal periapical healing can be observed where the contact with the canal filling material has been minimized [22].
Several methods can be used to establish the working length of the tooth, such as mathematical equations, predetermined norms of tooth length, electronic audio measurement, tactile sense, and so on; however, the most practical approach is to use an electronic apex locator (EAL) followed by confirmation of canal length by placing an endodontic instrument in the tooth [23], approximating the apex and verifying the accuracy of the instrument position with an undistorted radiograph during root canal treatment (Fig. 6.2.).
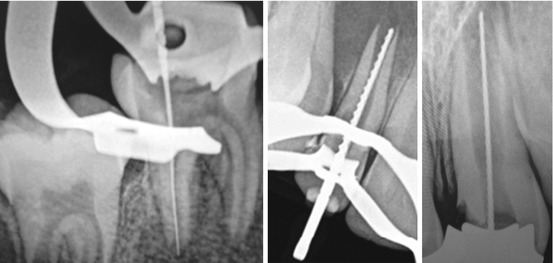
Fig. 6.2
Radiographs of files inside root canals to measure their length
The radiographic length is the length of the tooth as it appears on the radiograph [24]. The estimated working length is the radiographic length minus 1 mm [25]. The final working length is −1 mm subtracted from the anatomical apex measure from the working length radiograph [25].
The working length should never be solely based on EALs because although they are not prone to error with different irrigating solutions [26], their accuracy can be influenced by the presence of a nearby metallic restoration or vital tissue, the type of any electrolytes in the canals, the diameter of the apical foramen, an absence/presence of apical constriction, and the size of file used [27, 28].
Once a correct working length measurement is obtained, a reference point is established at the occlusal or incisal extension of the instrument and recorded [25]. This same working length is maintained throughout all of the endodontic preparation and filling procedures: the steps for the measurement of the canal system are:
-
The hand file used to take the diagnostic measurement will be set to the anatomical length using the measurement from the occlusal cusp height or incisal edge as a landmark to the radiographic apex. All radiographs should be of good quality, with minimal distortion and sufficient visible periapical area.
-
All subsequent file measurements will be set to the working length measurement which is the radiographic apex measurement minus 1 mm [25].
-
Clean the apical region without blocking the apical constriction or destroying the natural apical architecture
-
The purpose of using the anatomical length file is to maintain the patency of the apical region. If a radiograph shows a file length that is 2 mm or more from the radiographic apex, the file must be readjusted and a new x-ray taken to confirm the diagnostic length of the root canal.
-
Silicon or rubber stoppers are used to measure the instrument at the occlusal landmark. If these stoppers move, recheck their position against the designated landmark as you continue to clean the canal.
-
Instrumentation at the working length should continue to, at least, three instrument sizes above the file used to initially take the diagnostic measurement.
Final Instrumentation and Shaping the Root Canal
There is strong agreement that the adequate removal of necrotic and infected tissues is essential to the success of endodontic therapy [17]. However, there is seldom agreement on the optimum approach for the final instrumentation of the root canal. Over the years, it has become less acceptable to redesign the root canal space, and it should not be much larger than the original space or have a different center and angle to the original canal space [29]. A growing trend is to minimally alter the morphology and size of the original canal [30]. The root canals of the teeth are all unique, but they can share common dimensions and morphologies [31]. Once the root canal is negotiated to the apical third, a decision has to be made to continue with hand files or to use rotary NiTi instrumentation [10, 15].
At this stage the root canal has to be shaped, even if minimally altered, to facilitate the removal of necrotic and infected tissues and to provide space for placing the obturating materials [10, 15]. After years of experience, it has been learned that the best shape is one with a continuously tapering funnel from the canal orifice to the apex [1]. The reasons why this shape is recommended is it that it decreases the risks of procedural errors when cleaning and enlarging apically [32]. The size of root canal enlargement is often dictated by the method of obturation. For the lateral compaction of gutta-percha, the canal space should be enlarged to permit placement of the spreader to within 1–2 mm of the corrected working length [33]. There is a correlation between the depth of spreader penetration and the apical seal [34]. For warm vertical compaction techniques, the coronal enlargement must permit the placement of the pluggers to within 3–5 mm of the root canal working length [35]. There is a limit to the amount of shaping of a root canal, because the more that dentin is removed from the root canal walls, the weaker the tooth becomes [36]. The amount of root canal shaping is determined by the preoperative root dimension, the obturation technique, and the restorative treatment plan [10, 15]. Some narrow mandibular incisor roots cannot be enlarged to the same size as the more bulky roots of the maxillary central incisors. If the restored tooth requires a post to retain the crown, the canal space will need to be enlarged sufficiently to retain the post shown in Fig. 6.3.

Fig. 6.3
The left tooth has been instrumented and restored without a post; the right tooth has a post inside the root canal to hold a crown. The canal preparation in the right tooth is much larger to retain a post
Cleaning and Shaping to the Root Apex
The pulp and periapical tissue barrier can be determined histologically, but the barrier is difficult to accurately determine in radiographs. Since for mature teeth there is a need to retain files, instruments, sealers, and obturation materials within the root canal, it is necessary to terminate the cleaning and shaping of the canals at 1 mm before the radiographic apex of the tooth is reached [1, 10, 15]. The apical foramen or root apex is the narrowest portion of the root canal furthest from the crown. The morphology of the root apex can vary greatly from a tapering constriction to a multiple constriction, age and root resorption can add variation, and the foramen to apex distance can vary up to 3.8 mm [37]. The problem for cleaning and shaping the canal is to get as close to the apex as possible; otherwise, an uncleaned area of canal can harbor bacteria, but to still confine obturation to the root canal space [38]. Extrusion of the obturation materials must be prevented, and this must be planned at the root canal shaping stage.
Size of Apical Enlargement
Since the morphology of teeth can be highly variable, there is no generally regarded apical canal size. Minimal enlargement of the apical preparation is advantageous to limit canal transportation, but it can also decrease the effectiveness of the cleaning procedure to disinfect the canal. Apical transportation can be seen in most curved canals enlarged beyond a size #25 stainless steel file [39]. The most effective size of apical enlargement is the one which has adequately removed necrotic infected tissues. The apical root canal is the most difficult region of the canal to clean because of its constriction to irrigation, cleaning, and shaping. Some studies indicate that irrigating solutions are not able to reach the apical portion of the root if the canal is not enlarged to a size #35 or #40 file [40]. When the apical region is enlarged, it can significantly improve the disinfection of the root canal [41].
Shape and Size of the Instrumented Root Canal
The same design principle applies to both straight and curved root canals; they will be instrumented or prepared using a tapered design that is widest at the cervical level which gradually diminishes and ends at 1 mm before the root apex.
The taper of the prepared root canal is designed to allow the easy filling of the canal with obturation material and to condense the apical one-third of the canal with gutta-percha filling material [10, 15]. This taper is commonly called the “flare.” The minimal size of an instrumented or prepared straight canal should be to an ISO size 40 and a width of 1 mm. The maximum size is determined by the experience of the dentist to remove the necrotic infected tissues from the root canal. In curved canals, the amount of canal enlargement is determined radiographically and depends on the root direction and degree of curvature. In addition to negotiating calcified root canals and removing areas of resorption, the instrumentation size limitation is the mesiodistal thickness of the root canal walls, because it is essential to maintain the strength of the tooth.
Endodontic Hand File Geometries
Endodontic hand files (Fig. 6.4) are available in different lengths that are standardized by the American National Standards Institute/American Dental Association/ISO [42]. Most hand files have 16 mm of cutting flutes [10]. The cross-sectional diameter at the first rake angle of the hand file is termed D0. One-millimeter coronal to D0 is termed D1, while 2-mm coronal to D0 is called D2. The most shank-side cutting flute is 16-mm coronal to D0, which represents the largest diameter and most active cutting aspect of the instrument and is termed D16. Each hand file receives its numerical designation, or file name, from its diameter at D0. Since ISO files have a standard taper of 0.32 mm over 16 mm of cutting blades, the taper of any specific instrument is 0.02 mm/mm. Although each file name represents the size at its D0 diameter, each of the hand files has multiple cross-sectional diameters over its active blades. For example, The ISO size 10 file is 0.10 mm in diameter at D0, tapers 0.32 mm over 16 mm, and has a diameter of 0.42 mm at D16.

Fig. 6.4
Endodontic hand files
Endodontic Instruments
Nickel-titanium (NiTi) is a super elastic metal with a shape memory [43]. Endodontic NiTi rotary instruments were introduced in 1993 [44] and have changed the way root canal preparations are performed, enabling more complicated root canal systems to be shaped with fewer procedural errors [45]. The most commonly used type of NiTi instrument has a taper of .04 which is good for the cleaning of various canal types as shown in Fig. 6.5.
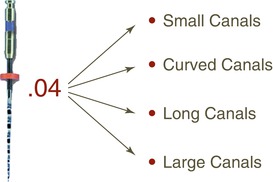
Fig. 6.5
NiTi endodontic instrument
NiTi rotary instruments have proved to be extremely successful for cleaning and shaping the root canals, but they should not be used when the dentinal walls are extremely thin to avoid perforation of the root canal. More than 30 types of NiTi instrument systems are sold, with varying designs, motors, shaping characteristics, breakage potential, and clinical performance [45]. The advantages of NiTi instruments are that they remain centered within the root canal space, thereby limiting its reshaping size, and that they bend only once per revolution, which lowers their risk of breaking. The manufacturers of endodontic instruments recommend that they only be used once, because their repeated use breaks the cutting tips (Fig. 6.6.) and lowers their cutting effectiveness.
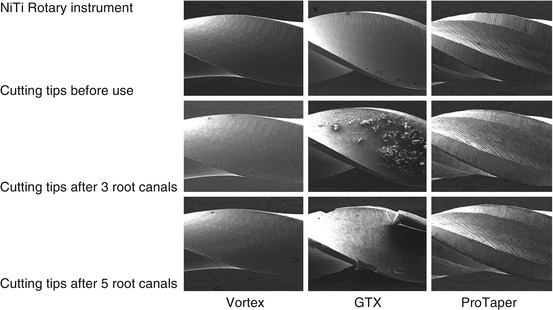
Fig. 6.6
Scanning electron microscopy of the cutting tips of endodontic instruments following repeated use
Using Hand Files and Instruments to Shape the Root Canals
The root canal cleaning and shaping goals require that the endodontic hand files and instruments must be used in sequential order from the smallest size first [1, 10, 15]. Throughout the treatment, from the initial hand file to the final canal preparation, it is necessary to maintain an accurate root working length by keeping an apical stop on the file so that the files and instruments are always kept within the confines of the root canal [25]. This will maintain the integrity of the tooth, avoid perforating the tooth, avoid injuring the periapical tissue, and minimize postoperative pain and discomfort for the patient. By obeying these goals, the original root canal will be enlarged, but not so enlarged that the tooth is weakened. The difference between the preoperative root canal and the postoperative root canal volume is shown in Fig. 6.7.
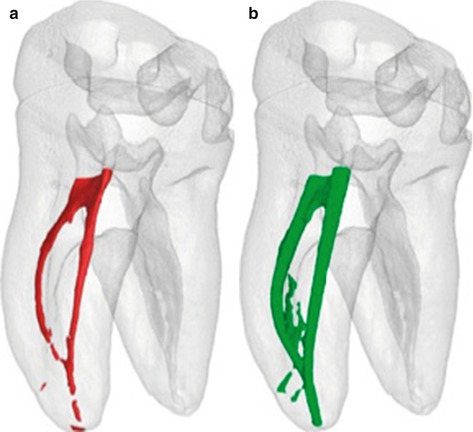
Fig. 6.7
Computer tomography of the root canal. (a) Preoperative root canal space. (b) Postoperative root canal space
Anti-curvature Filing
Curved canals are the most challenging to instrument, because the distortion of the files and instruments will cut into the curve to reduce its angle and place pressure on the cutting tips in an opposite direction, thereby increasing the risk of cutting a perforation [46]. The risk of cutting a perforation in curved canals increases when larger file sizes are used [46]. To avoid perforations, the concept of anti-curvature filing is to prepare a straight-line access through the root canal to the apical region, by filing away the bulky root structure to create a displacement space and by not touching the thin root walls which are in danger of being perforated.
Accessory Canals
Almost all root canals contain accessory canals. The presence of accessory canals has been a source of controversy as a cause of endodontic success or failure [47]. Accessory canals are of minimal importance to the outcome of endodontic treatment, provided that the main canals are adequately cleaned, shaped, prepared, filled, and sealed [48]. No effort is needed to locate accessory canals and to attempt to clean them; because of their small size, it is unlikely they can cause a flare-up and treatment failure.
Steps for Instrumenting the Root Canals
1.
The straight-line access opening should allow direct and unobstructed access to the apical region of the canal. A good access will minimize the torquing of the endodontic instrument and help avoid the perforation or stripping of the root canal.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


