Introduction
The role of the palatine tonsils in the development of dental intra-arch and interarch abnormalities is often brought up in the literature, but it remains controversial. Data on the probable relationship between enlarged tonsils and the occurrence of orthodontic abnormalities are subjective. The purpose of this study was to seek an association between the space occupied by the palatine tonsils and the dental arch measurements.
Methods
A cross-sectional study was performed on a group of children subdivided into 5 groups according to the standardized tonsillar hypertrophy grading scale. Dental arch measurements were recorded for each child. Data were analyzed with software. Comparisons of qualitative variables according to tonsillar grade were made using the chi-square test. The strength of the association between tonsillar grade and qualitative variables was evaluated with a phi coefficient (φ). The strength of the association between tonsillar grade and quantitative variables was assessed by the Spearman’ rank correlation coefficient (rho). The significance threshold was set at P = 0.05.
Results
The maxillary dental arch depth was significantly and positively correlated to grade. The maxillary intercanine, interpremolar, and intermolar widths were significantly and negatively correlated to grade. Grade 4 was strongly associated with molar Class II malocclusions, and posterior crossbite with functional lateral deviation of the mandible.
Conclusions
Early evaluation of the size of the palatine tonsils would help to prevent orthodontic abnormalities caused by upper airway obstruction. Thus, patients could be spared late, more aggressive treatments that are less efficient than treatments during childhood.
Highlights
- •
The higher the tonsillar grade, the lower the transversal dimension of the maxillary arch.
- •
Ratio of the depth of palatal vault to the maxillary interfirst molar width was correlated to grade.
- •
Grade 4 patients were more likely to develop a Class II than Grade 0 patients.
- •
Grades 3 and 4 patients were more likely to develop an open bite than grades 2 and 1 patients.
- •
Grade 4 was associated with a posterior crossbite with lateral deviation of the mandible.
The involvement of Waldeyer’s ring hypertrophy in the development of intra-arch and interarch dental anomalies is often brought up in the orthodontic literature, but it remains controversial. Most studies on this subject are based on 2-dimensional cephalometric evaluation of the pharyngeal diameter. However, it has been shown that the size of the palatine tonsils and the space they occupy in the pharynx airway are more determining than are the dimensions of the pharyngeal airway space. Thus, Brodsky and Koch have set up a tonsillar hypertrophy grading scale based on the space they occupy in the pharynx. However, to date, no study has been conducted to quantify the relationship between the space occupied by the tonsils in the pharyngeal airway and the intra-arch and interdental arch anomalies. The data in the literature on their probable relationship are subjective.
The main objective of this study was to seek a correlation between the space occupied by the palatine tonsils in the pharyngeal airway and the orthodontic anomalies that would support a prevention program for these anomalies at an early stage of dental arch development. A secondary aim was to determine from what grade the tonsils could be associated with orthodontic disorders.
Material and methods
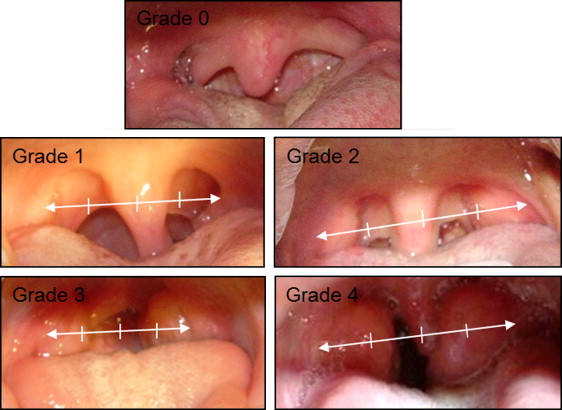
The patient sample consisted of 80 Senegalese children (37 boys, 43 girls) attending the Dento-Facial Orthopedic Clinic of the Department of Dentistry at Cheikh Anta Diop University in Dakar, Senegal. These children had undergone an initial ear, nose, and throat examination at the Department of Otolaryngology at the Fann University Hospital, Dakar, Senegal. They were divided into 5 subgroups according to their tonsil sizes. The different sizes were grouped into grades according to the standardized tonsillar hypertrophy grading scale of Brodsky and Koch. This grading scale is based on the space occupied by the tonsils between the anterior pillars of the oropharynx ( Table I ). Figure 1 clinically illustrates the different tonsillar grades.
| Grade | Definition |
|---|---|
| 0 | Tonsils limited to the tonsillar fossa |
| 1 | Tonsils occupying up to 25% of the space between the anterior pillars in the oropharynx |
| 2 | Tonsils occupying 25%-50% of the space between the anterior pillars |
| 3 | Tonsils occupying 50%-75% of the space between the anterior pillars |
| 4 | Tonsils occupying 75%-100% of the space between the anterior pillars |
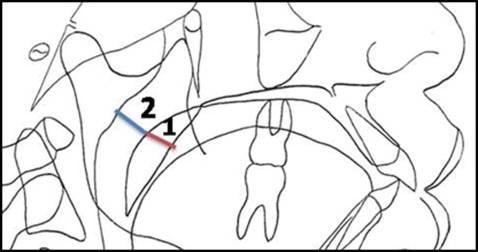
Boys and girls between 6 and 12 years of age were included in this study. Children who displayed any of the following were excluded: previous history of tonsillectomy, orthodontic treatment, nonnutritive sucking habits (finger, lip, tongue), chronic allergic rhinitis, nasal valve collapse, nasal septum deviation (diagnosed by endoscopy), nasal polyp (determined by nasofibroscopy showing grainy gray-yellow clusters in the nasal cavities), turbinate hypertrophy, hypertrophy of lingual tonsils (which abut both the rear side of the tongue and the posterior side of the pharynx), and obstructive adenoids (based on the radiographic method of Cohen and Konak, which compares the thickness of the soft palate with the pharyngeal airway space subjacent to it) ( Fig 2 ). These authors have shown it to be a reliable method, even on low-quality radiographs, and well correlated to other methods described in the literature.
On each selected patient, tonsillar grade was determined by the same observer (J.S.D.), who asked the patient to lie in a supine position, open his or her mouth wide, and continuously pronounce the phoneme /r/. At the same time, a tongue depressor was placed by the operator at the level of the posterior part of the dorsum of the tongue. The operator examined the pharynx without activating the gag reflex, making the tonsils rotate to bring them artificially closer to the median line.
On the basis of the ratio of the tonsils to the oropharynx (transversely measured between the anterior pillars of the pharynx), a standardized tonsillar hypertrophy grading scale was used ( Table I ). The percentage of space occupied by the tonsils between the anterior pillars of the oropharynx was thus determined after a direct intraoral examination ( Fig 1 ).
The following interarch parameters were noted or measured.
- 1.
Transversally: presence of a normal transverse occlusion, presence of a posterior crossbite with a functional lateral deviation of the mandible, and presence of a posterior crossbite without a functional lateral deviation of the mandible.
- 2.
Vertically: overbite (distance between the free edge of the maxillary central incisors and the free edge of the mandibular central incisors) and presence of a deep overbite, an anterior open bite, and a normal overbite.
- 3.
Sagittally: Angle molar and canine relationships and quantity of overjet.
The following intra-arch parameters were measured.
- 1.
Transversally: maxillary and mandibular intercanine widths (distance between the canine cusp tips); maxillary and mandibular interfirst molar widths (distance between the tips of the mesio-vestibular cusps of the first permanent molars); maxillary and mandibular interfirst premolar widths or interfirst deciduous molar widths (distance between the tips of the mesio-vestibular cusps of the first premolars or the first deciduous molars); ratio of the mandibular and maxillary interfirst molar widths; ratio of the mandibular and maxillary interfirst premolar widths (or the mandibular and maxillary interfirst deciduous molar widths).
- 2.
Vertically: total depth of the palatal vault (distance between the line joining the tips of the mesio-vestibular cusps of the maxillary first permanent molars and a point along the median raphe located in the aplomb); ratio of the depth of the palatal vault to the maxillary interfirst molar width.
- 3.
Sagittally: total lengths of the maxillary and mandibular arches (distance between the tangent line to the buccal surfaces of the central incisors and a tangent to the distal surfaces of the second deciduous molars or the second permanent premolars).
All dental arch measurements were made on plaster casts using an electronic caliper type of instrument (Mitutoyo, Tokyo, Japan) with precision of 2/100 mm, and resolution and reproducibility of 1/100 mm; the values were read directly in millimeters on the miniscreen of the caliper.
Statistical analysis
The collected data were analyzed using SPSS software for Windows (version 20.0; IBM, Armonk, NY). The strength of the association between the tonsillar grade and the quantitative dental measures was assessed by the Spearman correlation coefficient (rho). The chi-square test was used to compare the qualitative dental arch variables according to the tonsillar grade, and the strength of the association between these qualitative variables and the tonsillar grade was evaluated with a phi coefficient (φ). These strengths were analyzed using the values proposed by Cohen in 1988 ( Table II ). The significance threshold was set at P = 0.05.
| General interpretation of the strength of a relationship | r and phi (φ) |
|---|---|
| Very large | ≥0.70 |
| Large | 0.50 |
| Medium | 0.30 |
| Small | 0.10 |
Results
Eighty patients, 37 boys (46.3%) and 43 girls (53.7%), between 6 and 12 years of age (mean, 8.96 ± 1.88 years), were included in this study.
Table III shows a significant negative correlation between the age of the patients and their tonsil grades ( P = 0.009; rho = −0.29).
| Parameter | Grades (0, 1, 2, 3, 4) | |
|---|---|---|
| Rho | P | |
| Age | −0.29 ∗ | 0.009 |
For the assessment of quantitative dental arch parameters in the sagittal dimension, there was no significant correlation between the dental variables (overjet, total lengths of the maxillary and mandibular arches) and tonsillar grade. However, in the vertical plane, the total depth of the palatal vault was significantly and positively correlated to grade (rho = 0.44; P <0.001). Transversely, the maxillary intercanine width was significantly and negatively correlated to grade (rho = −0.34; P = 0.003). Likewise, the maxillary interfirst premolar width (rho = −0.34; P = 0.003) and the maxillary interfirst molar width (rho = −0.30; P = 0.007) were significantly and negatively correlated to grade. The ratio of the mandibular interfirst molar width to the maxillary interfirst molar width was also significantly correlated to grade, but the correlation was positive (rho = 0.30; P = 0.006). Similar results were found for the ratio of interpremolar widths and grade (rho = 0.29; P = 0.014). The combination of vertical and transverse dimensions shows a ratio of total depth of the palatal vault to maxillary interfirst molar width that was significantly and positively correlated to grade (rho = 0.65; P <0.001) ( Table IV ).
| Variable | Grades (0, 1, 2, 3, 4) | |
|---|---|---|
| Rho | P | |
| Sagittal dimension | ||
| Overjet (mm) | 0.026 | 0.819 |
| Total length of maxillary arch (mm) | 0.039 | 0.732 |
| Total length of mandibular arch (mm) | −0.169 | 0.134 |
| Vertical dimension | ||
| Overbite (mm) | −0.035 | 0.759 |
| Total depth of the palatal vault (mm) | 0.440 † | <0.001 |
| Transversal dimension | ||
| Maxillary intercanine width (mm) | −0.336 † | 0.003 |
| Mandibular intercanine width (mm) | 0.223 | 0.060 |
| Maxillary interfirst molar width (mm) | −0.297 † | 0.007 |
| Mandibular interfirst molar width (mm) | −0.107 | 0.343 |
| Maxillary interfirst premolar width or interfirst deciduous molar width (mm) | −0.340 † | 0.003 |
| Mandibular interfirst premolar width or interfirst deciduous molar width (mm) | −0.191 | 0.098 |
| Ratio of mandibular first molar width/maxillary first molar width (%) | 0.307 † | 0.006 |
| Ratio of mandibular first premolar width/maxillary first premolar width or ratio of mandibular first deciduous molar width/maxillary first deciduous molar width (%) | 0.286 ∗ | 0.014 |
| Vertical and transversal dimensions | ||
| Ratio of depth of the palatal vault/maxillary interfirst molar width (%) | 0.652 † | <0.001 |
For the assessment of qualitative dental arch parameters, comparisons according to grade showed significant differences from Angle’s molar relationship ( P = 0.015), Angle’s canine relationship ( P = 0.046), presence of anterior open bite ( P = 0.007), presence of normal overbite ( P <0.001), presence of a posterior crossbite with functional lateral deviation of the mandible ( P <0.001), and a normal transverse occlusion ( P <0.001) ( Table V ). The strength of the association between grade and these qualitative parameters was assessed by the phi coefficient (φ) equal to 0.558, 0.516, 0.419, 0.617, 0.595 and 0.671, respectively ( Table V ).


