This case report describes the treatment of a patient with a horizontally impacted maxillary central incisor, a canine in the same quadrant, and an inclusion tendency. Due to severe crowing in the maxilla and the Class II molar relationship on the impaction side, a 2-stage treatment plan was developed. In the first stage, the right first premolar and deciduous canine were extracted; this allowed enough space for the eruption of the maxillary right permanent canine. The second stage included surgical exposure and traction of the impacted central incisor with a fixed orthodontic appliance. An excisional uncovering technique was needed to expose the impacted incisor. After it erupted, an apically positioned partial-thickness flap was used to add keratinized attached gingiva in the area surrounding the crown, initially located in an area of unattached gingiva. The patient finished treatment with a normal and stable occlusion between the maxillary and mandibular arches and an adequate width of attached gingiva.
Impaction of a permanent tooth is not common in the mixed dentition; however, an impacted central incisor is usually diagnosed when the tooth fails to erupt. Although the maxillary canine is the most frequently impacted anterior tooth, impaction of the maxillary central incisor poses a problem at an earlier age. This tooth usually erupts several years before the canine, when the child is between 8 and 10 years of age, and its impaction is more conspicuous to the parents.
The most common causes of canine impactions are a long path of eruption, tooth size-arch length discrepancies, abnormal position of the tooth bud, prolonged retention or early loss of the temporary canine, trauma, an alveolar cleft, ankylosis, cystic or neoplastic formation, dilaceration of the root, supernumerary teeth, and odontomas. Although impaction of the maxillary central incisor is almost as prevalent as impaction of the canines, its etiology is different. The principal factors involved are supernumerary teeth, odontomas, and trauma. Adjacent anomalous or missing maxillary lateral incisors have been implicated in the etiology of palatally displaced canines by not providing proper guidance to the canine during its eruption.
Diagnosis of an impacted canine could occur before the age of 10 years if there is a family history or the maxillary lateral incisors are anomalous or missing, or after age 10 if there is asymmetry in palpation or a pronounced difference in the eruption of the canines between the left and right sides, or the canines cannot be palpated and occlusal development is advanced, or the lateral incisor is proclined and tipped distally, and, on a panoramic radiograph of the late mixed dentition, if the cusp tip of the canine overlaps the root of the lateral incisor.
Treatment alternatives for an impacted central incisor include extraction and restoration with a bridge or an implant later when growth has ceased; extraction and closure of the space by substituting the lateral incisor for the central incisor with subsequent prosthetic restoration; and surgical exposure, orthodontic space opening, and traction of the impacted central incisor into its proper position. Clinicians should consider treatment goals that minimize injuries to the dentition and the periodontium.
Resorption of the permanent incisors is a rare complication caused by ectopic eruption of the maxillary canines; when it happens, orthodontic treatment might be required. Sometimes, to reduce orthodontic treatment time and prevent further resorption of the maxillary central incisor roots, the impacted maxillary canines and mandibular first premolars are extracted, because of the proximity of the maxillary canine and central incisor roots.
Several factors might affect the outcome of the orthodontic-surgical plan for the resolution of impacted central incisors but, particularly, the manner in which the impacted tooth is exposed. Impacted teeth can be exposed by removal or repositioning the soft tissue that envelopes them, leaving them in full view at the end of the surgical procedure. This has been termed “open-eruption” exposure. Removal of the oral mucosa overlying the unerupted teeth, although more direct, has the disadvantage that the finally erupted tooth will have a nonkeratinized labial gingival margin, whereas apical repositioning can be expected to provide adequate width of the attached gingiva. The teeth might then erupt spontaneously, or, with a bonded attachment, an extrusive force can be applied to augment the diminished natural eruptive force.
However, little research has been carried out in the context of impacted central incisors until recently, when a study was undertaken to investigate the long-term periodontal, pulpal, and esthetic outcomes for a group of impacted maxillary central incisors exposed with a closed-eruption surgical and orthodontic treatment technique. Although the importance of a minimal zone of attached gingiva has been disputed, investigations have shown that an adequate zone of attached gingiva might prevent gingival recession. If the attached gingiva is too narrow, inflammation leads to recession rather than pocketing.
Diagnosis and etiology
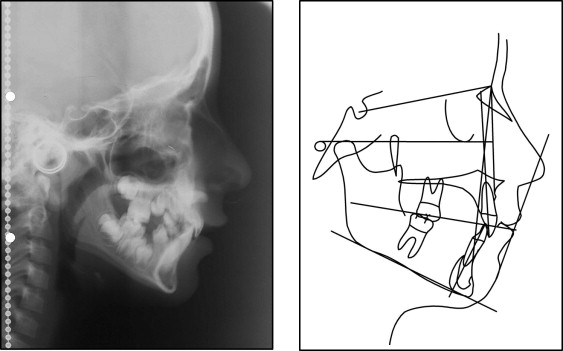
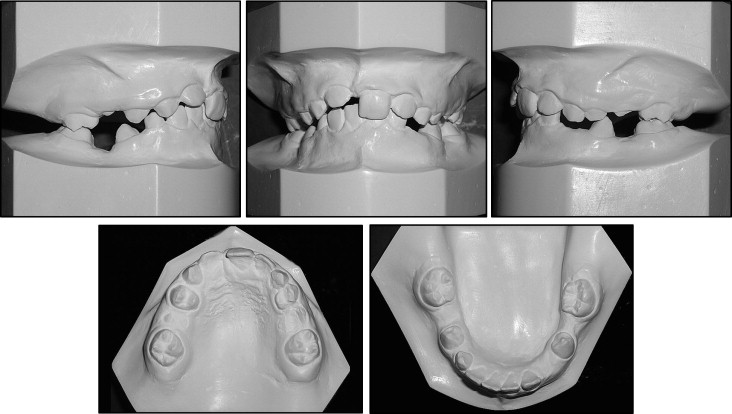
An 8-year-old girl in the early mixed dentition stage came with the appearance of her anterior teeth as her chief complaint ( Figs 1 and 2 ). She had a balanced facial pattern but an asymmetric smile, with the occlusal plane and upper lip canted upward to the right side and more gum showing on the left side. The maxillary dental midline deviated about 2 mm to the right. The maxillary right central incisor was impacted, and the adjacent teeth had drifted into the unoccupied space. There was significant dental crowding in the maxillary right arch with a Class II right molar relationship. Overjet was 2 mm and overbite 4 mm.

The patient had a history of trauma at age 4, with the premature exfoliation of some deciduous teeth. Radiographs showed that the maxillary right central incisor was impacted in a horizontal position in the region of the nasal floor, and the right canine had an impaction tendency (the incisal tip overlapped the root of the lateral incisor ) ( Fig 3 ).

Treatment objectives
The following treatment objectives were established: (1) recover space in the maxilla for the eruption of the right canine, (2) provide orthodontic traction for the impacted teeth, (3) create a stable functional occlusion, and (4) establish adequate attached gingiva and symmetric gingival margins for both maxillary central incisors.
Treatment objectives
The following treatment objectives were established: (1) recover space in the maxilla for the eruption of the right canine, (2) provide orthodontic traction for the impacted teeth, (3) create a stable functional occlusion, and (4) establish adequate attached gingiva and symmetric gingival margins for both maxillary central incisors.
Treatment alternatives
- 1.
Extraction of the impacted central incisor, orthodontic space opening, and future restoration with a bridge or an implant when growth had ceased.
- 2.
Extraction of the impacted central incisor and closure of the space, bringing the lateral incisor into the place of the central incisor, and subsequent prosthetic restoration.
- 3.
Orthodontic space opening, surgical exposure, and traction of the impacted dilacerated central incisor into its proper position.
Treatment plan
After discussing the possible treatment alternatives, the parents and the clinicians chose to try to save the tooth and bring it into its proper position. Because of the maxillary right canine’s impaction tendency, the treatment plan consisted of 2 stages. The first stage involved extraction of the right first premolar and the deciduous canine; the second stage consisted of fixed orthodontic treatment, surgical exposure, and traction of the impacted right central incisor from a horizontal to a vertical position and its alignment to obtain a normal occlusal relationship.
Treatment progress
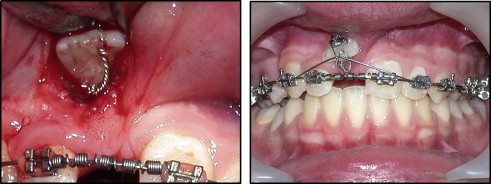
The maxillary right first premolar and deciduous canine were extracted to relieve crowding and facilitate canine eruption ( Figs 4 and 5 ). After the eruption of all premolars and canines, bands or brackets were placed on all teeth. Once the maxillary arch was in a relatively rigid stabilizing wire (0.018 × 0.025-in stainless steel in a 0.022-in slot), a coil spring was used to create adequate space for aligning the impacted incisor. Periodontal surgery was performed to expose the maxillary right central incisor ( Fig 6 ).