Digital technology has revolutionized the art and science of image capturing and processing. Clinical photography and radiology are 2 areas of orthodontics that are directly affected. But technology that makes it easier to acquire, store, view, and transmit images also makes it easier to alter them. This article briefly reviews the important aspects of digital forgery that are relevant to orthodontics, with special focus on how to recognize tampering and image authentication strategies.
Learn larceny, too, and then forget it. (Tamil aphorism, India)
Orthodontics has always proudly been in forefront to absorb new technologic advances for practical use. The widespread and passionate adoption of digital technology in orthodontic photography and radiography is an apt example. Digital cameras, digital radiographs, and image editing softwares are the order of the day. The orthodontic literature is replete with the technicalities and recommendations of these; no doubt an adequate knowledge of these is indispensable for their effective use. But with a high potential for misuse, it becomes equally important to know the methods in which they can also be abused. Recent reports on the increasing numbers of scientific articles containing questionable or falsified records have highlighted the vulnerability of scientific literature to digital forgery. This is also of critical concern to the specialty boards that approve digital case records for board certification examinations and the law courts that allow digital evidence in malpractice suits. These developments have thrown the issue of digital forgery into the limelight and amplified the need for prompt action.
The term digital forgery refers to all acts of unethical digital manipulation of images with the primary intent of altering their implications. The fakeness of an image can pertain to alteration of the original image in totality or in part by addition, removal, or masking modifications of specific characteristics of the image (eg, color, contrast), presentation under an altered context, splicing and blending several images into a composite, and combinations of the above.
Modifications of certain aspects of an image are permissible and even useful in certain cases. Adjustment of the contrast and brightness of a cephalogram image for better clarity and identification of landmarks is one such instance. Morphing an image (as done by orthodontic software) for patient education, growth prediction, and treatment prediction is a regular and accepted practice. But presenting the same image as the posttreatment photograph in any publication or board examination constitutes forgery. Therefore, it is the malicious intent that is more culpable than the nature of alteration or the generation process involved. Many scientific communities have earnestly attempted to provide guidelines on permissible limits in image editing, but a comprehensive policy with universal consensus is still elusive.
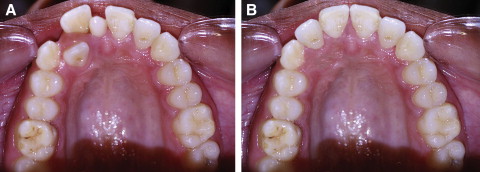
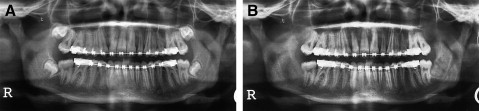
The alteration of an image acquired from a digital source (photographic or radiologic) by using image-editing software such as Photoshop (Adobe Systems, San Jose, Calif), Paintshop (Corel, Ottawa, Ontario, Canada), or others is the commonest and easiest method of generating a fake image. Figure 1 appears to show a patient’s pretreatement and posttreatment intraoral occlusal views. However, the posttreatment image was actually created from the pretreatment photograph by the following simple steps: the mesiodens and right central and lateral incisors of the original image were deleted, and the clone stamp tool was used to patch the soft-tissue environment. New right central and lateral incisors were created from their contralateral counterparts by mirror imaging and adjusted to fit as necessary. The edges of these pasted portions were smudged to make the merger indistinct to a casual viewer. Likewise, Figure 2 shows the original predebonding panoramic radiograph on the left and a tampered copy on the right; the copy was altered to simulate extractions of all third molars and the necessary root paralleling. The general availability and the relative ease of use of current digital cameras and graphic softwares have almost phased out the more demanding photo tricks of conventional photography required for such purposes.
The difficulty and complexity in identifying fakery in photographs is proportional to the level of precision and expertise involved. A carefully crafted fake image can fool even an expert in his or her field of dentistry. Although an absolutely fool-proof method to identify tampering is not yet available, certain visual and technical clues in the altered image can reveal the foul play.
Awareness of various methods of tampering and a critically suspicious appraisal are certainly the preliminary steps in identifying fakery. The presence of details altogether inconsistent with scientific logic should sound the alarm bell. Figure 3 shows an occlusal photograph of a mandibular arch with 3 incisors in the place of the mandibular left first and second premolars. This could possibly be presented as a rare case report, but the inconsistency with current scientific knowledge should spark the suspicion of an alternate possibility: a fake image.

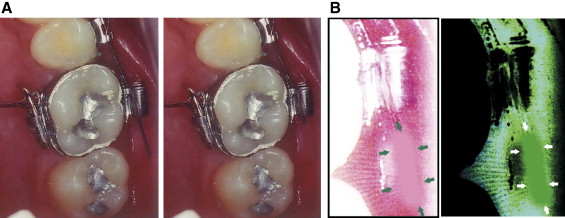
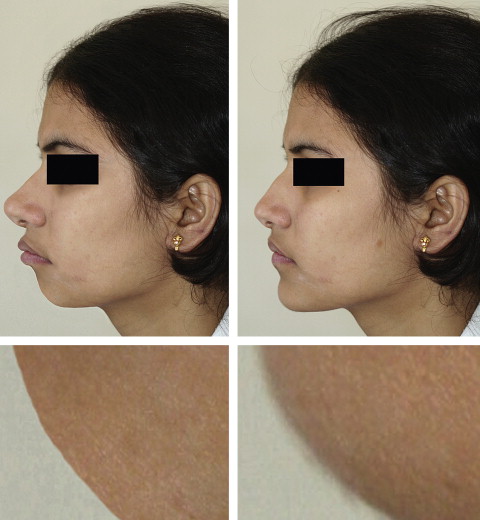
Zooming and close-up evaluation of an image might show the inconsistencies in image characteristics between the original and the tampered portions not otherwise visible at normal magnification. The more amateur the attempt at tampering, the more evident the imperfections. Figure 4 , A , shows a case with an excessively long distal end of the archwire (missed by the operator) and the manipulated image with the distal end masked. Although it is not obvious at normal magnification, the 135% zoom up of the region and the color-inverted section ( Fig 4 , B ) clearly demonstrate the attempted masking. As another example, Figure 5 , A , can be presented as the pretreatment and posttreatment profile photographs demonstrating drastic improvement in the facial esthetics achieved with surgical-orthodontic management. In reality, the posttreatment photograph is the original image from which the pretreatment image was created by scaling and distortion of the eyes, nose, mouth, and chin. A closer evaluation of one of the tampered area—the chin region—from the fabricated image ( Fig 5 , B , left) shows the unnaturally sharp and clear object outline, a telltale attempt at manipulation. Compare it with the naturally blurred and imperfect chin outline of the original image ( Fig 5 , B , right).
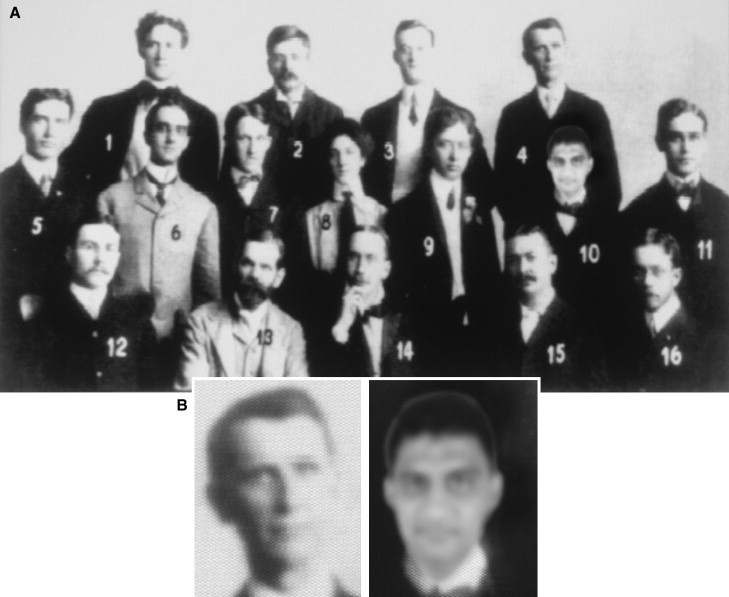
Inconsistency in the illumination characteristics between various parts of the image can be a sign of falsification when the illumination source, direction, and target morphology are well understood. Figure 6 , A , is the tampered photograph of candidates in Angle’s course of 1902, in which the head of the first author (B.M.) has replaced that of candidate number 10. Analysis of illumination conditions of the photograph shows that the light source should have been primarily from the left side of the members (shadows thrown on the right side). The close-up of the face of candidate 4 illustrates this clearly ( Fig 6 , B , left). The inserted face, however, has more uniform lighting created by balanced illumination from all sides ( Fig 6 , B , right). Such inconsistency in lighting conditions is a valuable clue to photo tampering. Also, note the mismatch between the tampered and the original portions with regard to image characteristics and pixelization, features not perceptible in Figure 6 , A , at normal magnification.
Inconsistency in perspective geometry is another clue to improper digital alteration. A careful analysis of Figure 3 shows that the incisors added to the photograph are geometrically inconsistent regarding emergence from the alveolus when viewed from this occlusal perspective. The inclination of other adjacent and contralateral posterior teeth appears to be normal, with their roots apparently extending into the alveolus. The added incisor crowns, however, are leaning too buccally. Assuming normal crown-root morphology, for such an inclination, their roots should be projecting out of the bone into the lingual vestibule as shown in Figure 7 . Thus, the tampering failed to maintain the perspective characteristics consistent with the occlusal view.



