Chapter 49 Hyoid suspension as the only procedure
1 INTRODUCTION
Obstruction of the airway at the retropalatinal and retropharyngeal airway is the key factor in the pathophysiology of obstructive sleep apnea syndrome (OSAS). Patient selection is crucial in successful surgery of the upper airway in OSAS. In addition to polysomnography, topical diagnostic work-up is of paramount importance in this regard. We routinely perform polysomnography first, and after that in cases of an Apnea/Hypopnea Index (AHI) below 30, schedule patients for sedated endoscopy (‘sleep endoscopy’) with midazolam (without an anesthetist present), in those patients in whom surgery is considered. In patients with an AHI > 30, who refuse NCPAP treatment upfront, or in patients who cannot accept NCPAP for whatever reason, sedated endoscopy is performed as well, but by an anesthetist, with propofol. In the study period (March 2000 to June 2004), in the case of mainly or only retrolingual obstruction, as assessed by sleep endoscopy and a low AHI (arbitrarily <15–20, snoring up to mild sleep apnea) we usually started with radio-frequent ablation of the tongue base. In this situation, in the case of mild or moderate OSAS, oral devices were offered as an alternative. In cases of a relatively higher AHI (moderate to severe OSAS), the effect of MRA treatment is less efficacious. In the case of an index of 15–30, and mainly retrolingual obstruction, we performed hyoid suspension (a.k.a. hyoidthyroidpexia) as the only procedure. In higher AHI patients we perform multilevel surgery (hyoid suspension, radiofrequency ablation of the tongue base, uvulopalatopharyngoplasty (UPPP), with/or without genioglossal advancement (see Chapter 17, Multilevel surgery). These patients usually have more severe and multilevel obstruction, which explains the higher AHI.
2 PATIENTS AND METHODS
2.2 UPPER AIRWAY ASSESSMENT
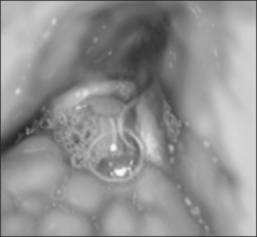
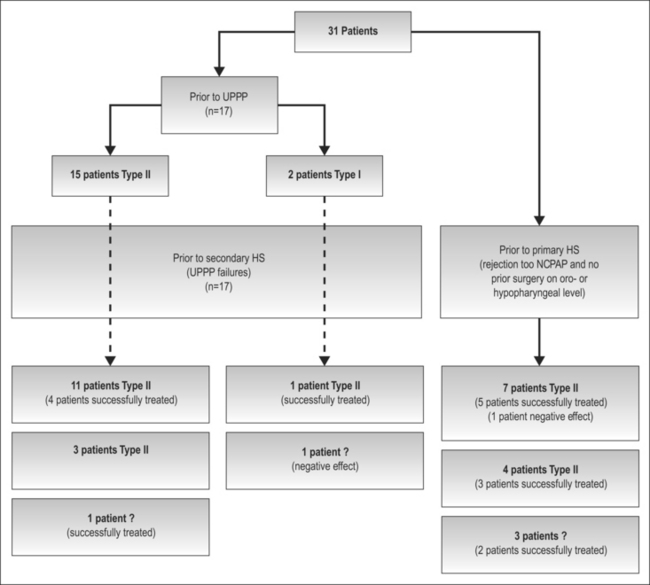
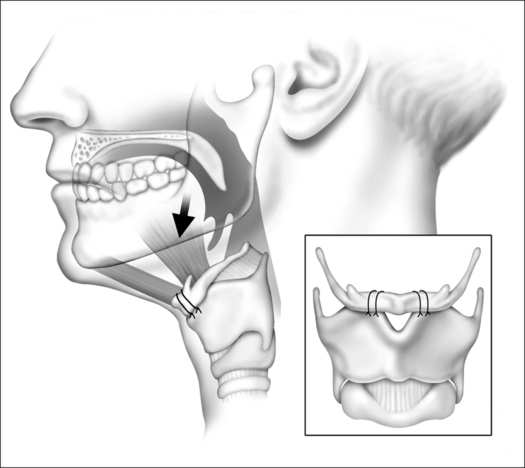
Hyoid suspension was performed in the case of obstruction at the base of tongue (Fig. 49.1), assessed by physical examination and flexible sleep endoscopy. A high suspicion of mainly retropalatal obstruction (large tonsils and long uvula) excluded patients for hyoid suspension. Candidates for surgery were categorized into two groups: those who did not have prior surgery at oro- or hypopharyngeal level (primary hyoid suspension); and those for whom UPPP was inadequate or detrimental (secondary hyoid suspension). In the latter group hyoid suspension was offered as salvage treatment. Multilevel obstruction (Fujita II) occurred in 20 patients; slight obstruction at retropalatal level in nine patients (primary hyoid suspension, n=14) and residual retropalatal obstruction after UPPP in 12 patients (secondary hyoid suspension, n=17). Only four patients who underwent primary hyoid suspension showed simple tongue base obstruction (Fujita III). Prior to UPPP, 15 patients showed multilevel obstruction (Fujita II), with emphasis on thepalatal level; two patients showed retropalatal obstruction only (Fujita I). Sleep endoscopy work-up according to the Fujita classification is shown in Figure 49.2.
3 SURGICAL TECHNIQUE
3.1 HYOIDTHYROIDPEXIA AND POSTOPERATIVE MANAGEMENT
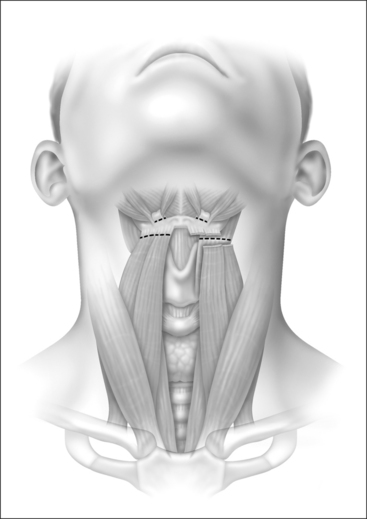
Under general anesthesia, with the head in a slightly extended position, a horizontal incision of approximately 5 cm is made in a relaxed skin tension line at the level between hyoid and thyroid cartilage (Fig. 49.3). Excessive fat tissue is excised, if helpful for better visualization. In the case of a further posterior positioned hyoid, removal of fat is recommended also, since otherwise the anterior placement of the hyoid will result in a somewhat turkey-like neck contour.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


