Introduction
This experimental study was designed to evaluate how the rate of dentoalveolar distraction into a bony defect affects bone quality and quantity.
Methods
Using 6 adult foxhound dogs and a randomized split-mouth design, we evaluated the differences between regenerate bone produced by distracting segments of bone containing the second premolars at either 1 or 2 mm per day for 5 days, followed by a 6-week consolidation period. Microcomputed tomography was used to evaluate bone density, percent bone volume, trabecular number, trabecular separation, and trabecular thickness.
Results
The lingual aspect of the regenerate exhibited more bone than did the buccal aspect, and all but one of the 12 specimens showed less than 1 mm of vertical bone deficiency in the regenerate area. No differences were found between the 1-mm per day and the 2-mm per day rates for bone density, percent bone volume, trabecular number, trabecular separation, and trabecular thickness. With the exception of trabecular separation on the 2-mm per day side ( P = 0.030), there were no statistically significant differences between the mesial, middle, and distal segments of the regenerate. Compared with control bone, the regenerate bone was less dense, and had less bone volume, a higher trabecular number, and approximately half the trabecular thickness.
Conclusions
Bone regenerate produced by rates of 1 and 2 mm per day of dentoalveolar distraction was similar in quality and quantity. Although less mature, the size and shape of the regenerate bone produced by rapid dentoalveolar distraction was comparable with the control bone.
Management strategies for treating edentulous spaces have been recently developed based on the principles of distraction osteogenesis. Distraction osteogenesis, which was introduced at the turn of the 19th century as a means of rapidly lengthening the lower extremities, uses osteotomies followed by a period of gradual separation of the bony segments. In 1973, the first distraction osteogenesis procedure was performed in the craniofacial complex to advance a mandible by 15 mm. Since that time, distraction osteogenesis has proven to be a viable option for augmenting bone in the oral cavity and the craniofacial complex.
In 1998, Liou and Huang used a distraction device attached to the teeth to rapidly move canines after surgical intervention. Their approach relied on the periodontal ligament to move the canines distally in 3 weeks. Ai et al, who performed the only animal study evaluating the biologic effects of periodontal distraction, showed that the distracted tooth moved twice as fast as the control tooth, with anchorage maintained, minimal root resorption, and little or no loss of bone. A few years later, Kisnisci et al introduced dentoalveolar distraction, a more invasive surgical approach based on osteotomies around the teeth, to move the segment of bone containing the canines distally. Iseri et al used this approach to move canines distally 1 mm per day in 8 to 14 days. Because it relies on distraction osteogenesis, dentoalveolar distraction might be expected to hold greater potential for generating bone than periodontal distraction. To date, no studies have evaluated the bone regenerate produced during dentoalveolar distraction.
The rate of distraction is a factor with important implications for a successful clinical outcome. Ilizarov was the first to introduce what has become the de facto standard rate (1 mm/day) of distraction used in most clinical situations; he showed that rates that are too slow produced a premature union, and rates that were too fast produced nonunion between the long-bone segments. Animal studies of mandibular distraction have shown greater stability and bone densities with a rate of 1 mm per day than with rates of 0.5 to 4 mm per day, even though bone fill was noted with the other rate groups. Craniofacial distraction has been carried out by using rates of 2 mm per day or even greater, with nonunion uncommon. The effects of the rate on bone regenerate quality and quantity after dentoalveolar distraction remain unknown.
There is presently no consensus as to the optimal rate for dentoalveolar distraction. This is partially due to our limited understanding of how rate affects the bone regenerate. On that basis, this study was designed to evaluate the quality and quantity in 3 dimensions of regenerate bone produced by 2 rates (1 mm/day vs 2 mm/day) of dentoalveolar distraction.
Material and methods
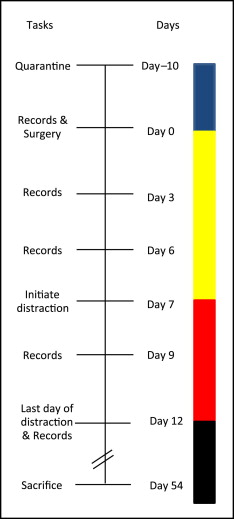
Six male periodontally healthy foxhound dogs, weighing 55 to 65 lbs and between 1 and 2 years of age, were used as the experimental model. The sample size was based on previous split-mouth designs demonstrating significant differences in tooth movements. The animals were quarantined for 10 days; then each dog received an ultrasonic dental prophylaxis. Initial records included alginate impressions, photographs, mandibular occlusal radiographs, and measurements of tooth positions. Notches drilled into the mesial aspect of the canine and the distal aspect of the second premolar served as stable references for repeated measurements with digital calipers. Occlusal radiographs were taken with the Nomad x-ray unit (Aribex, Orem, Utah) and Air Techniques digital radiographic sensors (Air Techniques, Melville, NY) with a number 4 size film. To measure the movements of the distracted segments, radiographs and measurements with calipers were taken before surgery, immediately after surgery, and on days 3, 6, 9, 12, and 54.
Triad custom impression trays were fabricated from a dry foxhound skull for initial alginate impressions. Impressions poured with improved dental stone were used to fabricate the distraction devices. Orthodontic band material (3M Unitek, St Paul, Minn) was used to custom-make bands to fit the mandibular canines and second premolars. Hyrax expansion screws (Dentaurum, Ispringen, Germany) were adapted to passively fit the contours of the bands and then soldered to the bands. The internal surface of each band was roughened with a number 2 bur (Brasseler USA, Savannah, Ga), and 3 holes were made through the band to increase mechanical retention. The appliances were then polished with pumice to ensure smoothness.
The inferior alveolar, lingual, and long buccal nerves were blocked by using 2% lidocaine with 1:100,000 epinephrine (Patterson Dental, St Paul, Minn) delivered through a 27-gauge needle. The dogs were initially sedated with a mixture of 2.2 mg per kilogram of body weight ketamine (Bioniche Teoranta, Galway, Ireland) and 0.22 mg per kilogram of body weight of xylazine (IVX Animal Health, St Joseph, Mo). After the initial sedation, the dogs were intubated and given 1% to 1.5% isoflurane (Butler Animal Health Supply, Dublin, Ohio) in oxygen at 1 L per minute. Atropine (0.05 mg/kg) (IVX Animal Health) was given subcutaneously to prevent bradycardia. After anesthesia was achieved, the mandibular first and third premolars were extracted.
After those teeth were extracted, a full thickness mucoperiosteal flap was reflected ( Fig 1 , A ), and a through and through vertical osteotomy was first performed 1 mm distally to the second premolar from the superior aspect of the alveolar ridge to within 1 mm of the mental nerovascular bundle. A similar cut was performed 1 mm mesially to the fourth premolar. These 2 vertical bony cuts were connected with a horizontal osteotomy 1 mm superior to the mental nerve and the inferior alveolar neurovascular bundle. The osteotomized segment of alveolar bone was separated from the lingual periosteum and completely removed from the ridge to mimic a long-standing periodontal defect or edentulous area. Another vertical osteotomy was performed 1 mm mesially to the second premolar and connected to the alveolar defect by a horizontal osteotomy inferior to the root of the tooth. The second premolar dentoalveolar transport segment was completely mobile except for the lingual mucoperiosteal attachment, which maintained the blood supply to the segment ( Fig 1 , B ).
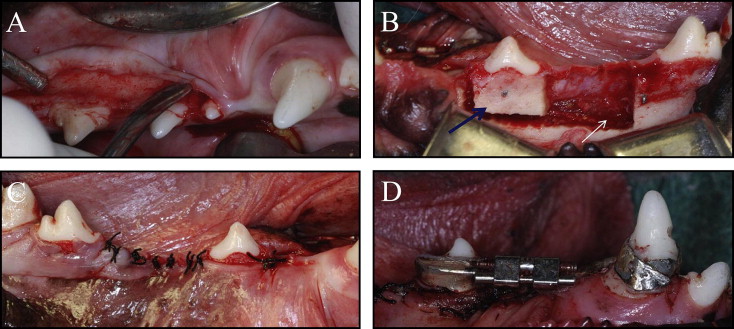
After wound closure ( Fig 1 , C ), the mandibular canines and second premolars were etched with 37% phosphoric acid gel for 30 seconds. All-Bond 2, primer A and B (Bisco, Richmond, British Columbia, Canada), was mixed and applied to each tooth; after 10 seconds, All-Bond 2 adhesive resin was applied and cured for an additional 10 seconds. The bands were filled with Filtek Supreme restorative composite resin (3M ESPE, St Paul, Minn) and seated onto the prepared teeth. Once the distractors were seated, light curing of the composite was performed for 40 seconds per tooth ( Fig 1 , D ). Due to extreme occlusal interferences, the maxillary canines of 2 dogs were sectioned 1 mm coronally to the band of the distracter, the pulp chamber was debrided, and Dycal calcium hydroxide (Dentsply International, York, Pa) was placed into the chamber and canal. The chamber was sealed with 3M Filtek Supreme composite (3M ESPE).
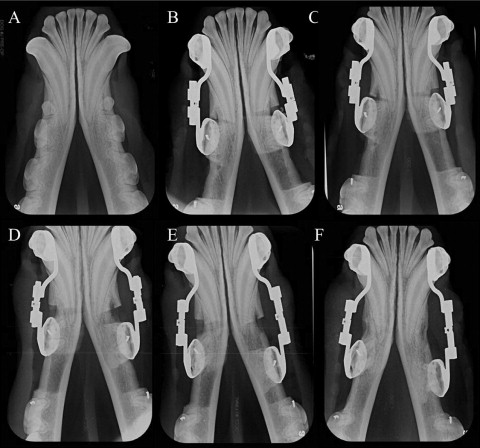
After a 7-day latency period, both sides were distracted for 5 days ( Fig 2 ). Distraction was performed at 2 rates. The right and left sides of the mandible were randomized, with 1 side distracted at 1 mm per day, and the opposite side distracted at 2 mm per day. The animals were sedated with ketamine and xylazine as before to obtain the radiographs and measurements.
After 6 weeks of consolidation (day 54), the dogs were killed, and the mandibles were disarticulated and sectioned. The specimens containing the regenerate bone, the dentoalveolar distracted segment, and the control alveolar bone were assigned random observation numbers and evaluated by a blinded examiner (A.C.S.). Specimen retrieval and data analysis are further described in a companion article by Moore et al.
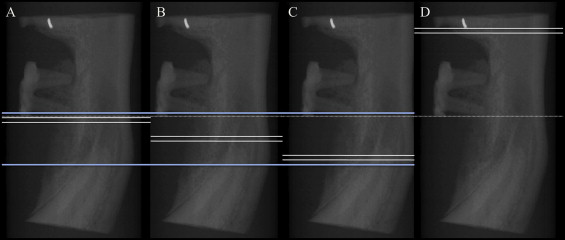
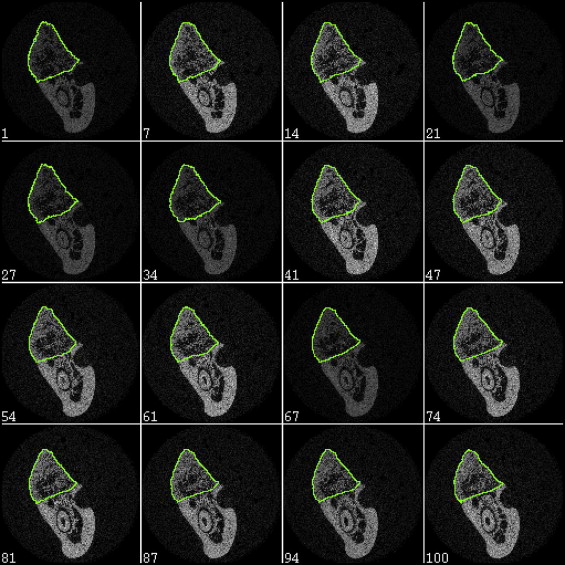
The specimens were placed in 27-mm long Scanco scanning tubes and loaded into the Scanco Micro-CT 35 scanner (ScanCo Medical, Bassersdorf, Switzerland). A preview radiograph was used for defining the segments of interest ( Fig 3 ). The entire specimen was then scanned at 60 μm to obtain an overall digital 3-dimensional (3D) reconstruction. Four additional scans were taken at a higher resolution (15 μm) for quantification of bone structure. The regenerate bone was divided into 3 volumes (mesial, middle, and distal), with each volume including 100 slices. The 100 slices used as control bone came from a continuous area of alveolar bone mesial to the fourth premolar. The regenerate regions of each volume and the comparable region of control volume were segmented by the examiner with the Scanco Micro-CT software (version 6.0) ( Figs 4 and 5 ). Scanco bone trabecular morphometry software was used to estimate bone density, bone volume fraction, trabecular number, trabecular thickness, and the space between trabeculae referred to as trabecular separation.
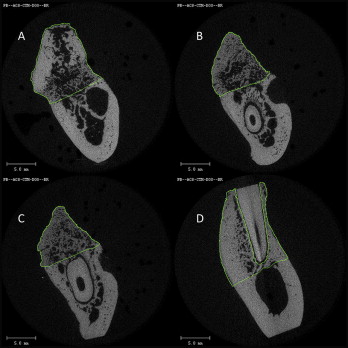
Using the 3D reconstructions and 2-dimensional individual slice images, additional assessments were made with a scaled ruler. The width of the regenerate was measured by using the occlusal view and compared with the adjacent control bone. Vertical bone height was measured at the middle of the regenerate by using the lingual view. Bone on the buccal and lingual aspects of the regenerate was compared with the buccal and lingual bone of the control bone. Finally, the buccal bone of the distracted segment surrounding the tooth was categorized as no bone loss, or mild (0-2 mm), moderate (2-4 mm), or severe (>4 mm) bone loss.
Statistical analysis
Statistical analyses were performed with SPSS software (version 15; SPSS, Chicago, Ill). Friedman tests were used to evaluate differences between the 3 regenerate sections, as well as for differences between all 4 sections. Nonparametric Wilcoxon signed rank tests were used to analyze differences between the 1-mm per day rate and the 2-mm per day rate sides.
Results
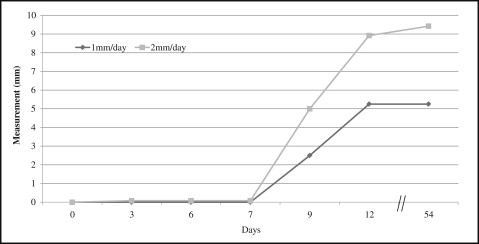
On average, the 2-mm per day side was distracted approximately 9.5 mm in 5 days, whereas the 1-mm per day side was distracted 5.3 mm ( Fig 6 ). Radiographic bone fill was evident at day 54 ( Fig 7 ). Two dogs experienced bond failures; both appliances were rebonded and reactivated within 24 hours.
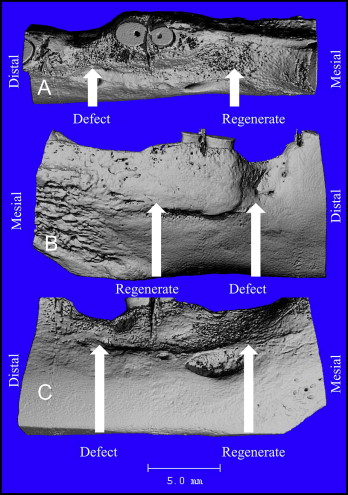
Upon gross inspection, the regenerate bone on both sides of the mandible had a more trabecular appearance than did the control bone. There were areas of mineralized cortical bone within the regenerate sections ( Fig 8 ). From the buccal view, 3 of the 12 specimens had mild bone defects remaining distally to the distracted segment, 5 showed moderate defects, and 3 showed a severe defect ( Table I ). From the occlusal view, all specimens showed little or no buccal bone loss, with none showing more than 2 mm of loss. Vertical bone deficits of the regenerate were noted in 10 of the 12 specimens, with 1 specimen showing a 2-mm deficit. From the buccal view, 1 specimen exhibited no loss, and 1 specimen demonstrated mild bone loss on the buccal surface of the distracted segment containing the tooth (both specimens were from the 2-mm/day group), 4 specimens showed moderate (2-4 mm) bone loss (2 from the 1-mm/day group and 2 from the 2-mm/day group), and 6 specimens displayed severe (>4 mm) bone loss (4 from the 1-mm/day group and 2 from the 2-mm/day group).
| Distraction rate | Estimated bone deficits (mm) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | 0.5 | 1.0 | 1.5 | 2.0 | 2.5 | 4.0 | 5.0 | 7.0 | |
| Buccal view of alveolar defect remaining distal to the distracted tooth | |||||||||
| 1 mm | – | – | 0 | 1 | 1 | 0 | 1 | 2 | 1 |
| 2 mm | – | – | 1 | 1 | 1 | 1 | 1 | 1 | 0 |
| Occlusal view of horizontal bone deficits of the regenerate | |||||||||
| 1 mm | 3 | 3 | – | – | – | – | – | – | – |
| 2 mm | 4 | 2 | – | – | – | – | – | – | – |
| Lingual view of vertical bone deficits of the regenerate | |||||||||
| 1 mm | 2 | 3 | 1 | – | – | – | – | – | – |
| 2 mm | 4 | 2 | 0 | – | – | – | – | – | – |
| Buccal view of vertical bone deficits of the regenerate | |||||||||
| 1 mm | 2 | 2 | 1 | – | 1 | – | – | – | – |
| 2 mm | 0 | 4 | 2 | – | 0 | – | – | – | – |
| Evaluation of bone deficits on the buccal surface | |||||||||
| None (0 mm) | Mild (<2 mm) | Moderate (2-4 mm) | Severe (>4 mm) | ||||||
| 1 mm | 0 | 0 | 2 | 4 | |||||
| 2 mm | 1 | 1 | 2 | 2 | |||||
The control bone was significantly different from the regenerate bone. It had approximately 25% more bone volume, 10% greater bone density, a 60% decrease in trabecular number, and a 50% reduction in trabecular thickness. Trabecular separation was not significantly different between the regenerate and the control bones ( Tables II and III ).
| Variable | Alveolar bone | Regenerate | Group comparisons | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Control | Distal | Middle | Mesial | Four | Three | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | P value | P value | |
| Bone volume fraction BV/TV (%) | 75.7 | 3.8 | 53.2 | 9.3 | 56.6 | 11.2 | 59.0 | 7.0 | 0.006 | 0.223 |
| Bone density (mg HA/cm 3 ) | 959.35 | 42.43 | 868.35 | 47.97 | 855.53 | 44.53 | 847.05 | 87.62 | 0.020 | 0.223 |
| Trabecular number (1/mm) | 1.62 | 0.12 | 2.31 | 0.22 | 2.42 | 0.24 | 2.57 | 0.68 | 0.014 | 0.115 |
| Trabecular thickness (mm) | 0.47 | 0.03 | 0.23 | 0.05 | 0.24 | 0.06 | 0.25 | 0.11 | 0.029 | 0.513 |
| Trabecular separation (mm) | 0.15 | 0.03 | 0.20 | 0.05 | 0.18 | 0.05 | 0.17 | 0.07 | 0.102 | 0.311 |
| Variable | Alveolar bone | Regenerate | Group comparisons | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Control | Distal | Middle | Mesial | Four | Three | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | P value | P value | |
| Bone volume fraction BV/TV (%) | 75.2 | 9.8 | 52.7 | 8.1 | 60.6 | 15.8 | 57.1 | 5.5 | 0.017 | 0.311 |
| Bone density (mg HA/cm 3 ) | 949.26 | 31.29 | 882.48 | 27.28 | 849.28 | 54.79 | 828.70 | 47.73 | 0.020 | 0.513 |
| Trabecular number (1/mm) | 1.54 | 0.31 | 2.30 | 0.45 | 2.53 | 0.66 | 2.86 | 0.18 | 0.007 | 0.311 |
| Trabecular thickness (mm) | 0.51 | 0.13 | 0.24 | 0.06 | 0.27 | 0.16 | 0.20 | 0.01 | 0.012 | 0.846 |
| Trabecular separation (mm) | 0.16 | 0.05 | 0.21 | 0.05 | 0.15 | 0.03 | 0.15 | 0.03 | 0.072 | 0.030 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


