Armamentarium
|
History of the Procedure
The earliest description of tongue lesions and their medicinal treatment is found in the Egyptian Papyrus Ebers from around 1550 bc . Between 600 and 300 bc , Sushruta described a surgical technique to treat macroglossia by rupturing a lingual cyst. In 1695, at an assembly of the Society of Medicine of Stockholm, a Dr. Hoffman performed what might be described as a partial glossectomy to treat severe macroglossia in a 10-year-old girl using a chisel and then cautery to control hemorrhage.
A description of tongue malignancy is notably absent from ancient medicine. The first case report of tongue cancer may be that of Ralph Freeman, who died of a tongue cancer on March 16, 1634. Much later, D’Arcy Power, an English surgeon, described an alarming increase in the incidence of “squamous” tongue cancer in late nineteenth-century England. He astutely observed that its rise seemed to coincide with the increased prevalence of tobacco use, although the common thinking at that time linked tongue cancer to syphilis. This increased prevalence coincided with the adoption of surgical management of head and neck cancers based on halstedian principles: complete primary resection en bloc with the adjoining lymphatic basins. Today, surgery remains the primary treatment of oral tongue malignancy.
History of the Procedure
The earliest description of tongue lesions and their medicinal treatment is found in the Egyptian Papyrus Ebers from around 1550 bc . Between 600 and 300 bc , Sushruta described a surgical technique to treat macroglossia by rupturing a lingual cyst. In 1695, at an assembly of the Society of Medicine of Stockholm, a Dr. Hoffman performed what might be described as a partial glossectomy to treat severe macroglossia in a 10-year-old girl using a chisel and then cautery to control hemorrhage.
A description of tongue malignancy is notably absent from ancient medicine. The first case report of tongue cancer may be that of Ralph Freeman, who died of a tongue cancer on March 16, 1634. Much later, D’Arcy Power, an English surgeon, described an alarming increase in the incidence of “squamous” tongue cancer in late nineteenth-century England. He astutely observed that its rise seemed to coincide with the increased prevalence of tobacco use, although the common thinking at that time linked tongue cancer to syphilis. This increased prevalence coincided with the adoption of surgical management of head and neck cancers based on halstedian principles: complete primary resection en bloc with the adjoining lymphatic basins. Today, surgery remains the primary treatment of oral tongue malignancy.
Indications for the Use of the Procedure
Tongue Dysplasia and Malignancy
Glossectomy is indicated for treatment of oral premalignant and malignant lesions of the tongue. The most common malignancy of the tongue is squamous cell carcinoma (SCCA).
The treatment of premalignant tongue dysplasia is surgical. Several nonsurgical therapies have been studied, including topical agents and systemic medications. None of these have led to long-lasting resolution of oral dysplastic lesions. Superficial partial glossectomy, taken just below the mucosa with minimal 5- to 10-mm margins, reduces but does not eliminate the risk of dysplasia recurrence. More important, it allows for pathologic review of the lesion and possible early identification of occult SCCA.
SCCA of the oral tongue is primarily treated by glossectomy. Radiotherapy has not been found to be as effective and has detrimental long-term side effects. Glossectomy can be done in the form of partial glossectomy, hemiglossectomy, subtotal glossectomy, or total glossectomy. Glossectomy is performed for SCCA with a 1- to 1.5-cm margin of grossly normal tissue, with the goal of obtaining at least a 5-mm pathologically clear margin. Some surgeons argue that “compartmental” resection of the entire muscle compartment leads to improved local control, although the data supporting this are limited to a few institutions. Radiotherapy with or without chemotherapy is used as an adjuvant when the tumor exhibits high-risk pathologic features, such as lymph node metastasis, perineural invasion, lymphovascular invasion, close or positive margins, or extracapsular extension.
In early-stage (T1 or T2) base of the tongue (BOT) SCCA, the advent of transoral robotic surgery (TORS) has allowed BOT partial glossectomy without open surgical approaches. TORS is indicated for BOT SCCA tumors that do not extend into the vallecula, that are not deeply infiltrative, are well lateralized, and that the surgeon expects to be able to remove with negative margins. Retrospective data reviewing outcomes from TORS for oropharyngeal SCCA followed by adjuvant radiotherapy with or without chemotherapy have found comparable local and regional control of disease but with improved swallowing function after treatment.
Macroglossia and Obstructive Sleep Apnea
Other indications for partial glossectomy include tongue reduction for macroglossia. Macroglossia is a component of several syndromes and systemic illnesses, such as Down syndrome, Beckwith-Wiedemann syndrome, amyloidosis, and congenital hypothyroidism. Treatment of obstructive sleep apnea may include median glossectomy as part of the treatment plan. Several surgeons have described various techniques for reductive glossectomy, aiming to reduce bulk but maintain mobility and function. These methods are discussed in other texts.
Limitations and Contraindications
A properly functioning tongue is essential for speech and swallowing, both of which are central to most social interactions. The most nuanced part of the treatment of tongue cancer is planning and executing the reconstruction to preserve these complex functions. Unfortunately, current techniques for doing so are comparatively simplistic and limited.
The critical features to recapitulate, in order of importance, are tongue mobility, anterior tip shape, size of the tongue, and sensation. Tongue mobility is most affected by the amount of remaining mobile tongue tissue. Resections involving up to 50% of the oral tongue can be replaced without soft tissue flaps with good retention of speech and swallowing function. Resections involving up to 75% of the oral tongue retain enough mobile tongue to maintain good function if the missing bulk is replaced with a soft tissue flap. Patients with subtotal and total glossectomy are more challenging. Before free tissue transfer, these were performed in conjunction with total laryngectomy due to high rates of aspiration from total glossectomy alone. Currently, these major defects can be reconstructed with soft tissue flaps that import enough bulk that movement of the mandible can create a neotongue-to-palatal seal. In this way, the patient can preserve airway protection. With regular therapy by a speech-language pathologist (SLP), intelligible speech and safe swallowing are achievable in most patients.
For BOT malignancy, surgery is limited by both the size of the primary tumor and by access. A large T4 BOT SCCA that extends deeply into the tongue musculature and encroaches on the oral tongue may require total or subtotal glossectomy to achieve clear margins. BOT SCCA can involve much more of the mobile root of the tongue, resulting in larger postoperative deficits in tongue mobility.
As described previously, surgical access to the BOT is invasive, and primary treatment by nonsurgical means is generally favored. If TORS is available and indicated, the key factor in deciding between surgical and nonsurgical therapies is the anticipated functional outcome. If BOT SCCA is thought likely to require adjuvant chemoradiotherapy, a nonsurgical treatment plan should be considered because the functional outcome probably will be equivalent with or without surgery.
Other than severe medical comorbidities, the only contraindication to glossectomy is the availability of alternative treatment that is less destructive and equally efficacious.
Technique: Partial Glossectomy of the Oral Tongue
Step 1:
Establishing a Secure Airway
Because of the risk of airway embarrassment from tongue swelling or hemorrhage, glossectomy is most often performed under general anesthesia. For T1 and smaller T2 oral tongue SCCA, intubation with a nasal right-angle endotracheal (RAE) tube often suffices. The tube is secured so that pressure on the nasal ala is avoided. Taping the tube to a Mayfield headrest or to a head drape with a foam pad placed on the forehead is generally effective.
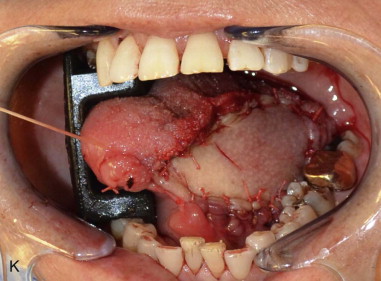
For larger SCCA (T3 or T4) or when a free flap is planned, a tracheostomy is often wise (see Chapter 97 ). Placement of an armored endotracheal tube in the tracheostomy during the procedure results in a lower profile than a tracheostomy tube and keeps the tubing away from the surgical field. The endotracheal tube is secured to the skin of the chest wall with 2-0 silk sutures in a mattress fashion ( Figure 99-1, A and B ).



Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


