Chapter 39 Fundamentals of minimally invasive radiofrequency applications in ear, nose and throat medicine
Ear, nose and throat (ENT) medicine currently has several different systems at its disposal for minimally invasive treatments which apply high frequency electric current to achieve a therapeutic effect. This chapter is intended to provide a survey of the technical fundamentals and tissue effects of such systems.
1 SYSTEM OVERVIEW
1.1 TYPE OF APPLICATION
Four types of application of high-frequency energy can be distinguished:
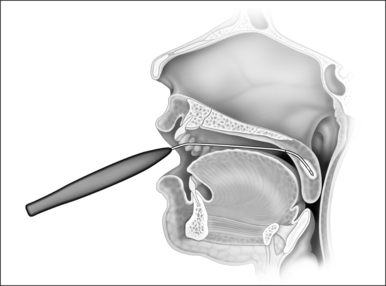
1.1.1 SUBMUCOUS COAGULATION
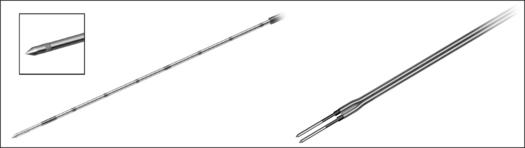
In the process of submucous coagulation, needle-shaped electrodes puncture the surface of the organ and are subsequently positioned inside the organ (Fig. 39.1). When energy is applied, thermally induced coagulation builds up around the electrode, usually of ellipsoid shape, depending on the construction of the electrode. If positioning and energy dose are correct, the organ’s surface is conserved and the application is almost entirely free of pain. The body’s own decomposition and discharge of the necrotic tissue leads to a reduction in volume in the region treated.
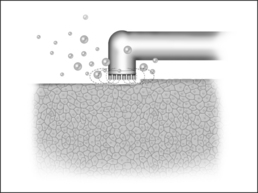
1.1.2 SUPERFICIAL VAPORIZATION
The reduction in size of an organ, e.g. a tonsil, may also be accomplished by means of direct tissue ablation via vaporization (tissue vaporization) on the surface (Fig. 39.2).
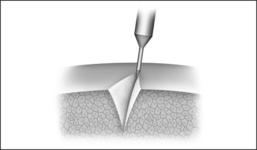
1.1.3 SUBMUCOUS VAPORIZATION
In the process of submucous vaporization, so-called ‘channeling’, channels are bored in the affected organ. For this purpose, a special bipolar electrode is necessary, at the tip of which a plasma ignition process takes place. When the tip comes into contact with tissue, the latter vaporizes immediately. A channel is generated by pushing the electrode forward in the tissue. More details on so-called plasma applications are to be found in Section 2.4.3.
1.2 THERAPY EFFECT
1.2.1 VOLUME SHRINKAGE BY THE BODY’S OWN DISCHARGE OF COAGULATION NECROSIS/TISSUE STABILIZATION BY SCAR FORMATION AFTER COAGULATION NECROSIS
Following thermo-coagulation several phases take effect in the volume of tissue involved.
1.3 EQUIPMENT TECHNOLOGY
1.3.1 MONOPOLAR AND BIPOLAR APPLICATION TECHNOLOGY
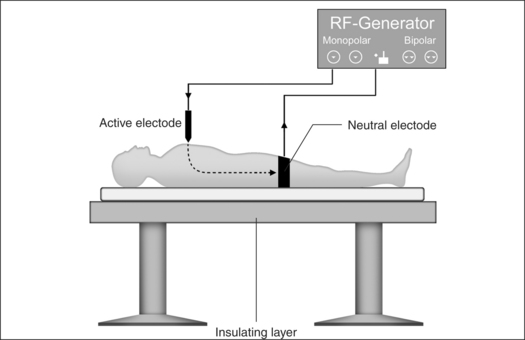
Monopolar technology
Monopolar technology, where one of the two electrodes required to close the circuit is connected to the patient as a large-surface return path, is most commonly used in radiofrequency surgical applications to date. The actual working or active electrode is in the shape of a small-surface surgical instrument, e.g. in the form of a needle, a lancet or a ball. It is from the latter electrode that the radiofrequency alternating current from the generator is conducted into the patient, producing the desired surgical effect as a result of high current density at the point where the tissue is touched. The radiofrequency current disperses rapidly in the tissue and flows with lower current density through the body of the patient to the neutral electrode, whence it flows back to the generator (Fig. 39.4).
A considerable number of complications may arise from the use of radiofrequency surgery, which are excluded when bipolar technology is applied.1
Problem: neutral electrode
Attachment of a neutral electrode to the patient is necessary when monopolar technology is used. In this context, attention must be paid to the certainty of low contact resistance. The current density has to be evenly distributed over the entire surface of the neutral electrode. Perspiration, hairs or fatty substances between skin and the electrode surface may mean the current is unable to utilize the entire transfer surface, leading to current densities which are too high in certain places and which may in turn lead to burns.2
Problem: current flow through the body between active and neutral electrode
Thermal tissue damage may occur in parts of the body between the active and neutral electrodes where the cross- section available for current flow is small and electrical resistance high.2 The current flow is particularly problematic in the region of head and neck: the greater part of the volume concerned here consists of bone as well as air-filled nasal and oral cavities or paranasal sinuses. In certain places only the thin mucous membrane layer remains as conducting residual cross-section.
The application of monopolar high-frequency technology for patients with cardiac pacemakers or catheters may only be carried out in exceptional cases. The specialist literature contains different documented opinions and research results on the interaction between radiofrequency current and pacemakers.3
Bipolar technology
Although bipolar technology has been known for some considerable time,4 it was only in the mid-1980s that renewed efforts were made to press ahead and further develop bipolar radiofrequency technology for reasons of safety, both for coagulation and cutting purposes.
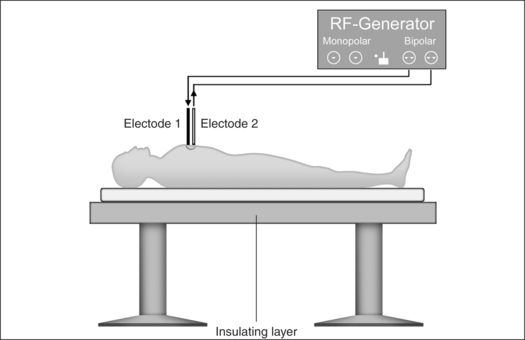
Bipolar application technology (Fig 39.5) is characterized in that both electrodes, integrated in an application handset, are brought as close together as possible. The current only passes immediately between the two electrodes, meaning that secondary thermal damage to the patient, both internal and external, caused by leakage currents or marked changes in impedance (cross-sections with a high percentage of bone or fat and poorly conducting residual cross-sections) can be avoided. Since the attachment of a neutral electrode is not required in bipolar radiofrequency surgery, and the current flow is restricted to the point of surgical intervention, the risks involved in monopolar technology as described above can principally be avoided (Fig. 39.6).
1.3.2 PROCESS MONITORING AND POWER REGULATION
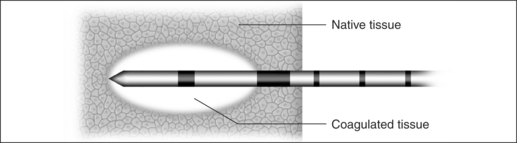
The size of a submucous coagulation (Fig. 39.7) depends on numerous parameters. Worth mentioning in this case are the electrode geometry, the power and the application time. Tissue resistance, tissue temperature or the energy input provide information on the tissue changes achieved.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


