Approximately 5% of patients presenting to a level 1 trauma center in the United States will have sustained basilar skull injuries. The etiology of frontobasilar trauma is variable but is often associated with severe multisystem trauma caused by the significant force necessary to disrupt the thick frontal bone. Nahum demonstrated in an experimental model that forces of 800 to 2200 pounds are required to fracture the frontal bone, a force more than 2 to 3 times that required to fracture any other facial bone. Neurologic injuries are therefore common in this population of patients. Cerebral contusion is generally the most common radiographic finding; however, subdural and epidural hematomas requiring operative intervention are present in as many as 10% of the patients. Open brain trauma, globe injury, cerebrospinal fluid (CSF) leak, frontal sinus disruption, frontonasal fractures, and frontotemporal-orbital fractures are common manifestations of frontobasilar trauma, and may require multidisciplinary management. Thus, contemporary management of frontobasilar trauma in the United States should occur at designated level I or II trauma centers, whenever possible, due to the availability in these centers of maxillofacial surgeons, neurosurgeons, and ophthalmologists.
Classification
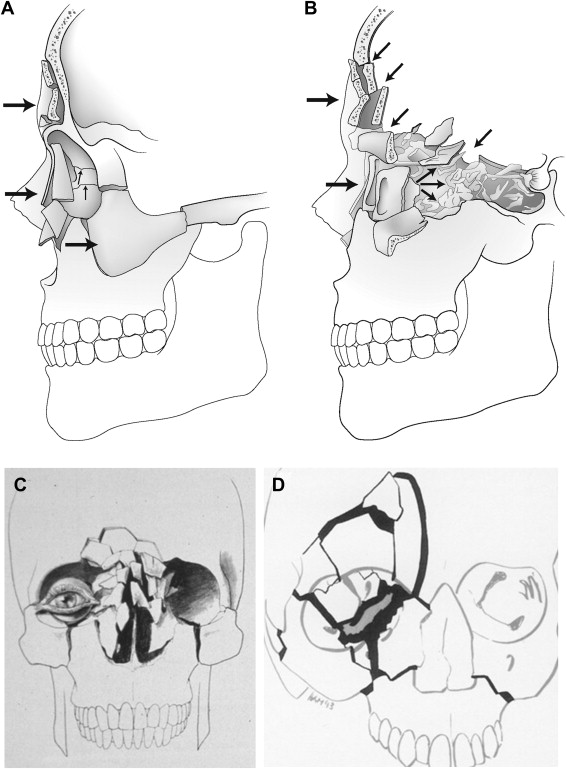
Several classification schemes have been advocated by various investigators in an attempt to describe injury patterns for frontobasilar fractures and to provide a clinically relevant decision-making tool. While a few are fairly descriptive of the injury components based on intraoperative and radiographic examination, most are too complicated to be clinically useful. The authors’ preferred classification scheme is that described by Raveh in 1992, which is based on the treatment of 355 patients with severe skull base and frontal bone involvement ( Fig. 1 ). In this classification the frontal, maxillary, and ethmoidal sinuses, the orbital cavity, and the nasal buttress may be regarded as shock absorbers, injury to which results in 2 broad injury categories: Type 1, which consists of frontonaso-ethmoidal and medial orbital frame fractures without skull base involvement; and Type 2, which consists of combined skull base, frontonaso-ethmoidal, and medial orbital frame fractures with frequent optic nerve compression. In Type 1 fractures, the external facial frame and buttresses give way and absorb and neutralize the impact, thereby preserving the posterior wall of the frontal sinuses, the frontal skull base, and the optic nerve canal. These injuries are not characterized by significant brain injury or dural laceration, and are generally managed by reduction of the external frame fractures and nasoorbital-ethmoidal component, if present, generally without the need for neurosurgical involvement. Type 2 fractures, on the other hand, are caused by high-energy forces that are not absorbed and neutralized by the external frame, and result in severe disruption of not only the external frame but also the internal palisades and buttresses. Type 2 fractures are characterized by intracranial dislocation of the posterior frontal sinus wall, inward telescoping of the nasal pyramid, and intracranial dislocations along the anterior skull base planes including the orbital roof and sphenoidal-parasellar areas. Significant neurologic injury is common, including dural tears, CSF leak, brain tissue herniation, intracranial hematoma, and optic nerve compression. Treatment often includes a subcranial or transcranial approach to remove (cranialize) the frontal sinus, repair underlying dural lacerations and, if indicated, decompress the optic nerve. Most Type 2 injuries require interdisciplinary cooperation between a maxillofacial surgeon and a neurosurgeon, and are in fact the subject of this article.