Introduction
In the course of orthodontic treatment with serial extractions (SE), spontaneous unraveling of crowded incisors occurs. It was hypothesized that SE followed by mechanotherapy will cause less external apical root resorption (EARR) than orthodontic treatment with late extractions (LE).
Methods
The records of 24 patients who underwent SE and mechanotherapy and 24 control patients who underwent LE and mechanotherapy were examined. The groups were matched for sex, central incisor root development and morphology, malocclusion class, ANB angle, and overjet. Lateral cephalograms taken before mechanotherapy (T1) and after mechanotherapy (T2) were traced and superimposed on the palatal plane with registration on the osseous details superior to the maxillary incisors and on the palatal curve. The T1 and T2 central incisor lengths, changes in the axial inclination, and horizontal and vertical apical movements were measured.
Results
The tooth lengths in both groups were reduced: the EARR values were 1.8 mm (± 1.1) in the SE group and 2.1 mm (± 1.4) in the LE group, and the difference between the groups was not significant. The movements of the teeth in both groups were similar in absolute values.
Conclusions
The spontaneous unraveling of incisor crowding with SE treatment does not prevent the common EARR seen in patients treated with LE, when the patients are treated by mechanotherapy after the SE.
External apical root resorption (EARR) is a common sequela of orthodontic treatment that is frequently discussed in the literature. The factors associated with this phenomenon are controversial. Among them are mentioned genetic background, length of treatment, magnitude of orthodontic forces, early vs late orthodontic treatment, type of orthodontic movement, trauma, and others.
Treatment with serial extractions (SE) has several advantages over the classic treatment regimen of orthodontic treatment with late extractions (LE) of 4 premolars. Among these, early attainment of the treatment goals and early application of mechanotherapy are mentioned. One study compared EARR in patients treated by SE followed by mechanotherapy with EARR in patients treated by classic LE of the 4 first premolars and mechanotherapy on the other teeth. The comparison was qualitative only and found that SE patients had somewhat less EARR, although it was not clinically significant.
The purposes of this project were to measure EARR in patients undergoing SE followed by mechanotherapy vs patients undergoing LE of the 4 first premolars and mechanotherapy, and to compare them. Our hypothesis was that patients in the SE group demonstrate less EARR because part of the tooth movement occurs spontaneously, without force application by orthodontic appliances.
Material and methods
For this retrospective controlled study, we used records from the long-term treatment registry at the University of Washington (IRB approval #23079).
The selection criteria for the subjects were the following.
- 1.
Class I crowded malocclusion.
- 2.
Four premolar extractions, either SE or LE during adolescence.
- 3.
Excellent quality records. Because periapical roentgenograms were not routinely taken (some patients had panoramic views for their initial or final records) and the long-cone technique was not always applied, and because of the great variability of the tooth-film relationships before and after treatment, it was decided to use the lateral cephalograms for the measurements of the length of the maxillary central incisors. Thus, only cephalograms of the highest quality were used in this study.
- 4.
Only patients with no history or evidence of tooth injury or wear, as shown on the charts and diagnostic records, were included.
A total of 59 SE patients were identified. Of these, 24 patients (19 girls, 5 boys) satisfied the selection criteria. Subjects were excluded (n = 35) because of missing or poor-quality records. A matched control group of 24 patients (17 girls, 7 boys), with 4 premolar LE followed by mechanotherapy, was selected from the same registry. These LE controls were matched with the SE group for age, sex, and ANB and overjet values before mechanotherapy (T1).
The following roentgenograms were used.
- 1.
Excellent-quality cephalograms before mechanotherapy (T1) and after mechanotherapy (T2). These were used for root-length measurements and superimpositions. The T1 and T2 cephalograms were traced in the same session and compared, so that cephalometric landmark locations were consistent. Special attention was given to the osseous details above the maxillary incisors and the palatal curve.
The orthodontist who traced the cephalograms (I.B.) could not be totally blinded to the patient’s group because in the SE group the T1 cephalograms were taken after the extraction of the premolars, and most (but not all) patients in the LE group had their cephalograms taken before extraction of the premolars.
- 2.
Periapical (PA) roentgenograms of the maxillary incisors at T1. These were found for 17 patients in the SE group and 20 patients in the LE group. The PA roentgenograms were used for evaluation of the developmental stage of the central incisors and any unusual root morphology.
- 3.
When the PA roentgenograms were missing, the T1 panoramic views were evaluated for the dental developmental stage of the maxillary central incisors.
To record the above parameters, the following measurements and evaluations were executed.
Tooth evaluation and baseline measurements were the following. (1) Root developmental stage at T1 (after Haaviko ): the relevant stages to this study were three quarters of the root completed, root completed but not closed, and apex closed. (2) Root morphology at T1 (after Levander and Malmgren ): 0, normal; 1, unusual: blunt, short, apical bend, pipette shaped. This evaluation was performed on the available PA radiographs for 72 teeth (of a total of 96 teeth for both groups). (3) Tooth length: tooth length of the maxillary central incisor at T1 and T2 was measured on the cephalograms from the incisal edge to the apex. When a difference in the length of the 2 adjacent maxillary central incisors was evident, the shorter root length was recorded. (4) Baseline measurements of ANB angle, overjet (along the occlusal line), and overbite (perpendicular to the occlusal line) at T1 were made on the cephalograms.
Change in root length (EARR) of the maxillary central incisor was recorded as the difference between tooth lengths from T1 to T2.
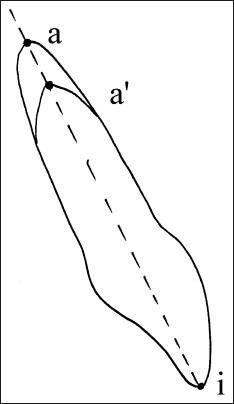
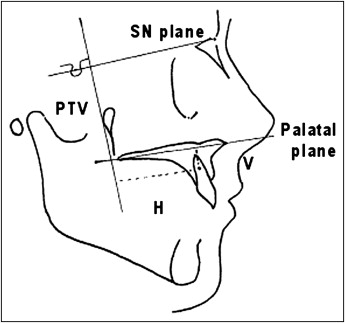
Maxillary incisor movements were measured as the following. (1) The axial inclination of the maxillary central incisor to SN (1/SN) between T1 and T2. (2) The vertical and horizontal distances that the maxillary central incisor root was moved during orthodontic treatment. Because EARR was observed in most subjects, the original apex of the maxillary central incisor at T1 could not be used for evaluation of root movement. Thus, the T2 apex of the central incisor was marked on the T1 superimposed central incisor image and named a′ ( Fig 1 ). The vertical and horizontal distances of the maxillary central incisor root movement during treatment were measured on the superimposition of the T1 and T2 tracings by using a′ ( Fig 2 ), denoting the same point on the T1 and T2 root. The superimposition was performed on the palatal plane with registration on the osseous details superior to the maxillary incisors and on the palatal curve. The measurements were made to the palatal plane (vertical component of movement) and to a perpendicular to SN through the pterygomaxillary fissure (horizontal component of movement).
All measurements were made to the nearest half millimeter and half degree.
Three weeks after the initial tracings and measurements, all cephalograms were retraced and remeasured to determine the reliability of the measurements and evaluations.
Statistical analysis
For categorical variables, numbers and percentages were calculated. For continuous variables, ranges, medians, means, and standard deviations were calculated. The Shapiro-Wilk test was used to analyze the normality of the distributions. The chi-square test was used to determine the association between categorical variables (a parametric test) or the Fisher-Irwin exact test (a nonparametric test for small numbers of observations). Pairs of categorical variables were compared by the Wilcoxon paired sign test. Pairs of continuous variables were compared with t tests. The 2-sample t test for differences in means was used to compare the subgroups (unpaired). All statistical tests were analyzed to a significance level of 0.05.
Results
Double determinations indicated good agreement between the 2 measurements in both groups at both time points. The exception was overbite at T1 (difference, 0.25 mm; P = 0.001). Since this difference was clinically acceptable, the mean values of the double determinations were used for all variables.
The distribution of the evaluation of the morphology of the maxillary central incisor (normal or deviated) was similar for all maxillary incisors in both determinations for the SE and LE groups ( P = 1). Thus, the first determination was used for further evaluations.
The 2 groups were matched ( Table I ) for sex ( P = 0.505) and chronologic age at T1 ( P = 0.341). Good agreement was also found for the ANB angle ( P = 0.343) and overjet at T1 ( P = 0.478). Overbite, however, was statistically significantly deeper in the SE group compared with the LE group, a difference of 0.7 mm ( P = 0.0332).
| Parameter | SE group | LE group | P value |
|---|---|---|---|
| Male/female ratio | 5/19 | 7/17 | 0.505 |
| Mean age at T1 (y) | 12.4 (1.5) | 12.8 (1.5) | 0.341 |
| ANB (°) | 3.0 (1.8) | 3.4 (1.3) | 0.343 |
| Overjet (mm) | 3.3 (1.28) | 3.6 (1.5) | 0.478 |
| Overbite (mm) | 3.4 (1.4) | 2.7 (1.0) | 0.0332 |
| Duration of treatment (mo) | 16.0 (8.7) | 17.8 (6.3) | 0.464 |
| Deviant root morphology | 11.2% | 10.5% | 1.000 |
| Tooth length (mm) | 27.1 (1.9) | 26.8 (1.2) | 0.442 |
The statistically insignificant difference of 0.4 year in chronologic age at T1 did not affect the dental developmental age of the incisors because all patients in both groups had the roots of the maxillary incisors completed, and only 1 patient in each group had roots completed but apices not closed at T1.
As expected, the mean duration of the fixed-appliance treatment was somewhat longer (by 1.8 months) in the LE group. This information was available for 20 patients in the SE group and for 17 in the LE group, and the difference was not statistically significant ( P = 0.464).
Root morphology of the maxillary incisors at T1 was normal in most subjects. Because of incomplete records in the SE group, only 34 teeth could be evaluated for this parameter; we found that 11.8% (4 of 34) of the central incisors showed some deviation such as dilacerations or pipette-shaped roots. A similar percentage (10.5%, 4 of 38) of central incisors with a deviant root form was found in the LE group for the 38 teeth for which this parameter could be determined. There was no difference ( P = 1) in this regard between the groups.
The tooth lengths at T1 in both groups were similar: 27.1 mm ± 1.9 in the SE group and 26.8 mm ± 1.2 in the LE group ( P = 0.6312). In both groups, the lengths were reduced at T2 ( Table II ): 25.2 mm ± 2.2 in the SE group and 24.8 mm (±1.9) in the LE group. Tooth lengths in the 2 groups were not statistically different at T2 ( P = 0.442).


