(1)
Dept. of Oral and Maxillofacial Surgery/Oral Pathology of the VU University Medical Center/ACTA, Amsterdam, The Netherlands
1.1 Examination of the Oral Cavity
1.1.1 Inspection
Examination of the oral cavity requires a proper source of illumination. The patient should be situated in a comfortable way, and there should be an adequate headrest device. Partial or full dentures should be taken out in order to allow proper inspection of the borders of the tongue and the floor of mouth in particular.
To be able to properly inspect the buccal mucosa, the use of two dental mirrors or cheek retractors is advised (Fig. 1.1). A piece of gauze enables to carefully grasp the tip of the tongue and to properly inspect the dorsal surface and the borders of the tongue as well as the floor of the mouth (Fig. 1.2).
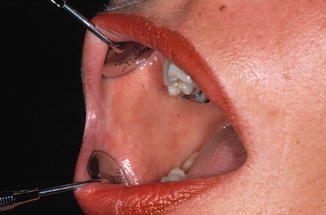

Fig. 1.1
Inspection of the buccal mucosa using two dental mirrors
Fig. 1.2
Inspection of the borders of the tongue with the use of a piece of gauze
In evaluating a mucosal lesion, one should not only observe the extent and the texture of the lesion but also its color. There may be some advantage in using special light devices (e.g., a fluorescent light source) or special dyes, e.g., toluidine blue, for the detection of early cancerous lesions.
In case of a lesion of the mucosal lining of the jaws, a radiograph may be required in order to assess possible changes in the underlying bone.
It is beyond the present treatise to discuss how to examine the neck. It is, of course, well recognized that a swelling in the neck, particularly a cervical lymph node metastasis, may lead to the detection of an oral or oropharyngeal squamous cell carcinoma.
1.1.2 Palpation
Manual palpation with gloved hands is an important part of the inspection of a mucosal lesion since it gives information about the consistency of the lesion, including the possible presence of induration. Such induration may indicate the presence of a malignancy.
Inspection of a lesion of the lips, the buccal mucosa, and particularly of the floor of the mouth may require bimanual palpation (Fig. 1.3).

Fig. 1.3
Bimanual palpation of the floor of the mouth
1.1.3 Exfoliative Cytology
The diagnostic value of exfoliative cytology in oral mucosal lesions is rather limited. Particularly in case of a suspected malignancy, a confirmatory biopsy remains required to establish a more reliable diagnosis.
1.2 Referral to a Specialist
1.2.1 When to Refer?
In general, each patient in whom the practitioner is unable to diagnose an oral lesion, either in the soft tissues or in the jaw bones, should be referred to a specialist, irrespective of the suspicion of malignancy.
Occasionally, a patient insists on being referred to a specialist (“a higher echelon”), while there is actually no need for it. In such instance, there is not much use in trying to prevent such referral.
1.2.2 To Whom to Refer?
The referral should be directed to a colleague with recognized knowledge and experience in that particular field, irrespective of the specialty of that colleague. For instance, in some parts of the world, an oral medicine specialist or a maxillofacial surgeon may be the appropriate colleague to refer to, while in other parts of the world, the dermatologist or the otolaryngologist may be the proper colleague for a given problem. In general, family doctors have had limited training in the diagnostic and therapeutic aspects of oral lesions and, therefore, are usually not the appropriate colleagues to whom to refer a patient with an oral problem.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


