The face is a complex and dynamic structure that must be carefully evaluated before any surgical intervention. Appreciation of the composition of the soft tissues, the importance of supporting skeletal and dental structures, and the interrelationship between static and functioning positions adds to the complexity. Compounding this complexity is the effect of the growth and aging process of the facial tissues. Surgical intervention at any time during the life cycle makes changes based on the surgical time referent, but other natural effects continue to mold the result over time. Understanding the predicted soft- and hard-tissue changes occurring during life is critical for surgeons responsible for making facial changes.
It is the purpose of this chapter to discuss the contributions of soft tissues and skeletal and dental structures to facial appearance and to provide insight into the evaluation of each, including the effects of aging on the soft tissues and skeletal and dental supporting structures. Also included in this chapter is a section on facial growth.
This chapter is divided into four basic sections: clinical evaluation of the face, cephalometric evaluation of the facial skeleton, evaluation of the occlusion, and evaluation of facial-skeletal growth. In each of these sections I will discuss evaluation in a pragmatic fashion. At the end of each of the first three sections I will conclude with a discussion of how the various tissues of the face change with aging.
It is of relevance that not every patient seen undergoes all four levels of evaluation. Level 4, Facial Skeletal Growth, is obviously confined to those younger than 18 years of age. Similarly, when an adult with a retrusive mandible is being evaluated, the performance of the Detailed Regional Facial Features assessment is relevant only with regard to the perioral evaluation. Also, most patients who undergo cosmetic facial surgery are candidates for an inclusive clinical evaluation of the face but not usually a level 2, 3, or 4 evaluation.
In sum, the specific concerns and patient presentation guide the judicious use of the four levels of evaluation discussed herein.
Finally, a brief evaluation of the face form is used to record only abnormalities detected during these examinations.
CLINICAL EVALUATION OF THE FACE
The clinical evaluation of the face is the most important of all evaluations of the face because the clinical evaluation is always the primary determinant of basic treatment recommendations.
Clinical examination of the face is separated into four basic evaluations: facial skin type, facial skin health, general facial anthropometric proportions, and detailed regional facial evaluations, such as the periorbital, nose, and perioral areas.
EVALUATION OF FACIAL SKIN TYPE
Although different proposals have been made over time with regard to classification of skin type, the Fitzpatrick skin typing system is the standard. This skin typing system categorizes skin as type 1 through type 6, based primarily on skin color and the skin’s response to sunshine. To simplify skin typing, Table 1-1 is used. The importance of skin typing relates primarily to the following practical matters:
- •
Level of sun protection recommended for the patient
- •
Patient’s susceptibility to actinic photodamage (aging)
- •
The modalities of therapy that are appropriate for the patient’s type of skin
| Skin Type | Skin Color | Characteristics |
|---|---|---|
| I | White | Always burns, never tans |
| II | White | Usually burns, tans less than average |
| III | White | Sometimes mild burn, tans about average |
| IV | White | Rarely burns, tans more than average |
| V | Brown | Rarely burns, tans profusely |
| VI | Black | Never burns, deeply pigmented |
For example, skin type 1 is extremely sensitive to actinic photodamage, and therefore individuals with this type of skin ideally would use a higher sun protection factor (SPF) sunscreen daily for sun protection. Moreover, with a skin type 5 or 6 it would not be generally recommended that CO 2 laser resurfacing or deep chemical peels be done, owing to the high incidence of problems with hypopigmentation and/or hyperpigmentation.
EVALUATION OF FACIAL SKIN HEALTH
Skin health has had several proposed methods of classification; I prefer the Glogau system. This system was proposed many years ago and basically evaluates cumulative actinic photodamage (i.e., DNA-induced cellular damage of the skin). It consists of types I through IV, where type I is mild and type IV represents severe skin damage. Table 1-2 summarizes the salient aspects of this system. Although additional aspects of skin damage assessment exist in the original Glogau system, three factors are primarily evaluated to determine the level of skin damage:
- •
The presence or absence of palpable and visible keratoses
- •
The degree or extent of dyschromia present
- •
The degree of loss of elasticity and therefore existing wrinkling and/or skin laxity
| Damage | Description | Characteristics |
|---|---|---|
| Type I | “No wrinkles” |
|
| Type II | “Wrinkles in motion” |
|
| Type III | “Wrinkles at rest” |
|
| Type IV | “Only wrinkles” |
|
Although generalities exist concerning age-related skin damage as noted with the system, more importantly the severity of facial skin damage is related to the cumulative exposure to ultraviolet radiation (UVA-UVB). Accordingly, a 35-year-old’s skin can be more severely affected than a 65-year-old’s.
GENERAL FACIAL ANTHROPOMETRIC RELATIONS
The esthetic facial evaluation is done directly on the patient, with the patient standing or seated comfortably and in the natural head position.
Frontal Face Evaluation
General Facial Characteristics.
Symmetry, balance, and morphology are the three major elements necessary for good front face esthetics and are sequentially evaluated.
Symmetry.
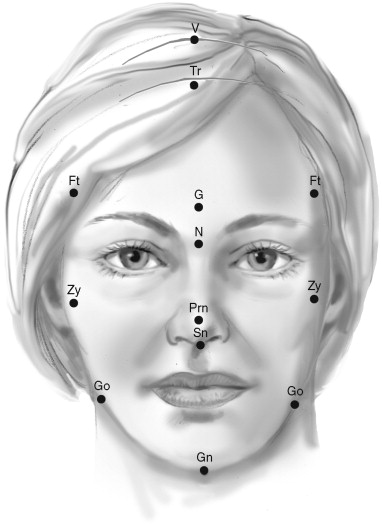
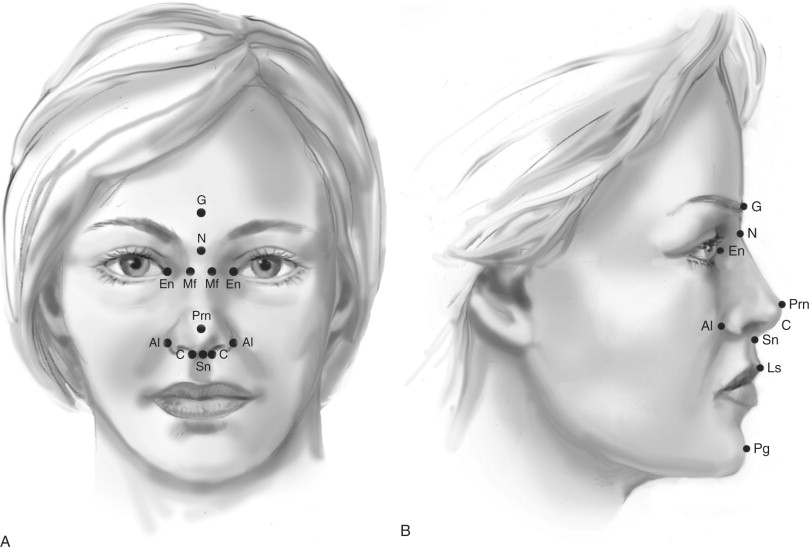
Although no face is perfectly symmetric, the absence of obvious asymmetry is important for good facial esthetics. Points Gn, Sn, Prn, N, and G should all be compatible with one another on the midline perpendicular to the horizontal referent ( Figure 1-1 ). In general, with a midline facial referent, points Ft, Zy, and Go right and left are accessed. When facial asymmetry is identified, the subsequently described detailed regional evaluations are used to better define its specific nature and amount.
Balance.
The total facial height is defined by the distance from points trichion (Tr) to gnathion (Gn) and may be divided into facial thirds by points glabella (G) and subnasale (Sn) (see Figure 1-1 ). The upper, middle, and lower facial thirds are defined as the distance from trichion to glabella, glabella to subnasale, and subnasale to gnathion, respectively. The ratios of the upper, middle, and lower facial thirds to the total facial height in an attractive person are 0.30, 0.35, and 0.35, respectively. Abnormal values are noted.
Morphology.
More important than categorizing a face as brachiocephalic or dolichocephalic, all facial thirds—upper, middle, and lower—are optimally of the same basic morphologic configuration in any individual. The morphology of each facial third is determined by dividing its width by the total facial height (see Figure 1-1 ).
The widths of the facial third are measured between three pairs of points bilaterally. The forehead width is defined by the distance between the frontotemporale (Ft) points—the slight elevation of the linea temporalis on either side of the forehead. The width of the middle third of the face is defined by the distance between the zygion (Zy) points—the most lateral points of the zygomatic arch. The distance between gonia (Go) bilaterally determines the width of the lower third of the face (see Figure 1-1 ). These horizontal measurements (bitemporal, bizygomatic, and bigonial), when divided by the total facial height (Tr-Gn), produce ratios of 0.65, 0.75, and 0.66, respectively.
The bizygomatic width is normally the greatest facial width, and the bigonial width is only slightly greater than the bitemporal width. Ratios larger than the norm indicate a short and/or wide tendency, whereas those smaller than the norm indicate a long and/or narrow tendency for the specific facial third being assessed.
Profile Evaluation
Upper Third of the Face.
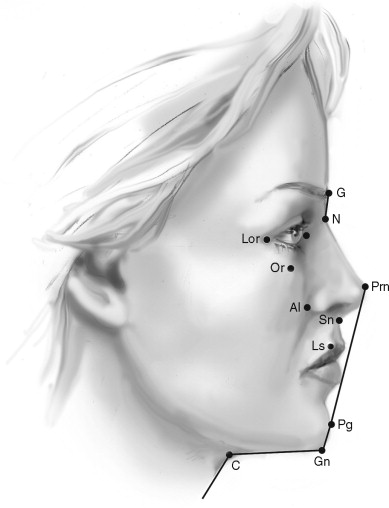
The upper third facial area esthetic examination considers primarily the shape of the forehead. The forehead is normally shaped such that it has an anterior slope from superior to inferior with an accentuation or projection of the supraorbital rims ( Figure 1-2 ). As with all periorbital structures, the projection of the supraorbital rims is primarily evaluated relative to the globes. Normally the supraorbital rims project 5 to 10 mm beyond the most anterior projection of the globe. When variations in the shape of the forehead and position of the supraorbital rims exist, the distinction is made between frontal bossing and supraorbital hypoplasia.
Middle Third of the Face.
The middle third facial area esthetic examination is subdivided into three areas: nose, eyes, and cheeks.
Nose.
Profile examination of the middle third of the face begins with an assessment of the nose. The nasal bridge projects 5 to 8 mm interiorly to the globes (see Figure 1-2 ). The nasal dorsum is described as normal, convex, or concave in appearance. The appearance of the nasal tip is evaluated for both the presence and absence of a supratip break and the direction of the nasal tip rotation, turned either up or down. Differentiation is made between a dorsal hump and a downturned nasal tip, because although these two conditions are similar in appearance on casual examination, their implications for treatment are different. The skeletal nasal base furnishes support for the alar base of the nose.
The ratio of the linear distance in the horizontal plane from the nasal tip (Prn) to the subnasale (Sn) and from the subnasale to the alar base crease (Al) is normally 2 : 1 (see Figure 1-2 ). Values approaching 1 : 1 are suggestive of lack of nasoskeletal support for the alar base and imply maxillary and/or middle third facial deficiencies. The nasolabial angle is normally between 90 and 110 degrees. This angle is defined as that formed between imaginary lines tangent to the columella (C) and the upper lip vermilion (Ls) and intersecting at the subnasale (Sn). When this angle is abnormal, one must distinguish between an upper lip posture problem and an abnormal columella angulation. For this reason, it is best also to use the relations of the upper lip to the subnasale perpendicular as a guide in determining protrusion or retrusion of the upper lip and dentition. Additional values relative to nasal esthetics appear in the section on the detailed regional evaluation of the nose.
Eyes.
The lateral orbital rim (LOR) normally lies 8 to 12 mm behind the most anterior projection of the globe, whereas the infraorbital rim (OR) is normally 0 to 2 mm anterior to the globe (see Figure 1-2 ). Values greater than these in the posterior direction are indicative of midfacial deficiency.
Cheeks.
The cheek, or area beneath the lower eyelid prominence, is normally convex. A flat to concave appearance is suggestive of midfacial deficiency. In older patients one can observe a double convexity, with relative fullness of the lower eyelid then a concavity around the level of the orbital rim and then a second convexity. This can be secondary to herniation of orbital fat and/or hypoplasia of the inferior orbital rim.
Lower Third of the Face.
Sequential observation in the lower third of the face includes the lips, labiomental fold, chin projection, and cervicomental area.
Lips.
The protrusion or retrusion of the upper lip is described as it relates to the subnasale perpendicular, an imaginary line through the subnasale and perpendicular to the Frankfort horizontal. The most prominent portion of the vermilion of the upper lip (LS) is +2 mm (see Figure 1-2 ). Normally the upper lip projects slightly (2 mm) anterior to the lower lip in repose. Protrusion or retrusion of each lip is independently noted because this most commonly relates to the underlying dental support.
Labiomental Fold.
A discernible labiomental fold gives definition to the lower half of the lower third of the face. The lack of a noticeable labiomental fold or an excessively deep fold detracts from this pleasant definition.
Chin Projection.
Chin projection is primarily related to the nose and subnasale perpendicular in the middle third of the face and the lips in the lower third of the face. Numerically its prominence is 2 to 6 mm behind the subnasale perpendicular, assuming normal nasal and maxillary prominence. It is important to note that the chin projection must be related to the entire profile to determine if it is adequately balanced with the forehead, cheeks, paranasal areas, and neck.
Cervicomental Area.
The cervicomental area can be subdivided into three areas of observation: mandibular angle–inferior border definition, neck-chin angle, and neck-chin length (see Figure 1-2 ).
Mandibular Angle–Inferior Border Definition.
The mandibular angle and inferior border are ideally well defined in profile, with a subtle but definite submandibular depression inferiorly. Skin laxity, cervical facial lipomatosis, parotid hypertrophy, and an excessively high mandibular skeletal plane angle are common conditions that obscure this definition.
Neck-Chin Angle and Length.
The neck-chin area normally exhibits an obtuse angle (110 degrees), and the distance from the pogonion to the neck-chin angle is approximately 50 mm. The presence of these relations gives definition to the chin and cervicomental area. The excessively obtuse neck-chin angle or deficient neck-chin length decreases this definition. The same factors that predictably obscure the mandible also unfavorably affect the definition of the neck-chin angle. In addition, chin deficiency contributes to an unaesthetic cervicomental area.
DETAILED REGIONAL FACIAL FEATURES
Six areas of the face will be discussed with respect to their more detailed evaluations. These are the periorbital area, cheeks, nose, perioral area, ears, and cervicofacial area.
Periorbital Area
When the periorbital area is being evaluated, numerous aspects of this will be quantified; however, the following are subjectively evaluated.
- •
Symmetry of the brow and eyes: The vertical symmetry of the inner and outer canthi is recorded. Generally a true horizontal line will bisect the inner and outer canthi of both eyes. A common malrelation, lateral canthal dystopia, occurs when the outer canthi are inferiorly positioned. Finally, ocular muscle imbalance, sclera discoloration, and the presence of sclera showing between the lower eyelid and pupil are assessed. The last item is commonly associated with skeletal deficiency in the midfacial area and/or lower eyelid retraction or ectropion.
- •
Shape of the brows: In males the brows are lower and more horizontal. In females the body arches upward from the head of the brow and then the tail drops inferiorly. Specific relationships are noted in Figure 1-3 .
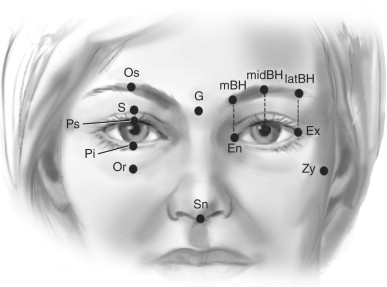
FIGURE 1-3 Periorbital anthropometrics. To view a color version of this illustration, refer to the color insert section at the back of this book.Vertical Proportions Orbit height/upper face height Os-Or/G-Sn 50% Upper lid height/orbit height Os-Ps/Os-Or 40% Eye fissure height/orbit height Ps-Pi/Os-Or 35% Lower lid height/orbit height Pi-Or/Os-Or 25% Sulcus to brow/orbit height S-Os/Os-Or 25% Sulcus to brow/lower lid height S-Os/Pi-Or 50% Sulcus to upper lid margin S-Ps 8-10 mm Upper lid margin to iris Ps/Iris 2 mm Lower lid margin to iris Po/Iris 2 mm Medial brow height/orbital height MBH/Os-Or 50% Mid brow height/orbital height MIDBH/Os-Or 55% Lateral brow height/orbital height LATBH/Os-Or 50% Horizontal Proportions Biocular width/head width Ex-Ex/Eu-Eu 60% Intercanthal width/biocular width En-En/Ex-Ex 34% Fissure width/intercanthal width En-Ex/En-En 95% Fissure width/biocular width En-Ex/Ex-Ex 33% Intercanthal width/zygomatic width En-En/Zy-Zy 25% Interpupillary width/biocular width Mid Pupil/Ex-Ex 70% Eye fissure cant/horizon En-Ex/horizon 5% Vertical/Horizontal Proportions Orbit height/biocular width Os-Or/Ex-Ex 35% Orbit height/fissure width Os-Or/En-Ex 95% Fissure height/fissure width Ps-Pi/En-Ex 35% - •
Presence or absence of redundant skin (dermatochalasis or blepharochalasis of the upper and lower eyelids) and a visible upper eyelid sulcus.
- •
Upper and lower eyelid fat excesses (herniation).
- •
Lower eyelid laxity (snap test).
Anthropometrically, examination of the eyes and orbits begins with measurements of intercanthal and interpupillary distances. The mean values and standard deviations for the intercanthal and interpupillary distances in Caucasian adults are 34 ± 4 and 65 ± 4, respectively. Increased intercanthal distance is telecanthus; increased interocular distance is ocular hypertelorism. The norms are slightly larger for dark-skinned people. These values are established by 6 to 8 years of age.
Proportions and Ratios.
The orbit height (Os-Or) is 50% of the middle facial height (G-Sn) (see Figure 1-3 ). the brown height (MIDBH) is 50-55% that of the orbital height (Os-Or). Within the orbit proper, the upper lid height (Os-Ps) is 40%, the eye fissure height (Ps-Pi) is 35%, and the lower lid height (Pi-Or) is 25%. These measure approximately 14 mm, 12 mm, and 10 mm, respectively.
Both eyelids overlap the iris by approximately 2 mm, and the upper lid sulcus is approximately 8 mm from the lid margin.
Horizontal relations reveal that the overall width of both eyes (Ex-Ex) is 60% that of the head (Eu-Eu). The intercanthal (En-En) and fissure widths are approximately equal (En-Ex), and these are 25% of the bizygomatic width (Zy-Zy).
Vertical/horizontal proportions are such that the orbital height (Os-Or) and fissure width (En-Ex) are approximately equal at 95% ( Figure 1-3 ). Additional vertical and horizontal relations are noted in the legend to Figure 1-3 .
Cheeks
Evaluation of the cheeks consists of sequential assessment of the cheeks proper (C) or malar eminences and infraorbital rims, paranasal areas (P), and buccal area (B) for symmetry and normal projections ( Figure 1-4 ). Several views are useful in this assessment, including the three-quarter oblique and profile views. The malar eminences are normally present 10 to 15 mm lateral and 15 to 20 mm inferior to the lateral canthus. These measurements are taken using an imaginary x,y coordinate system originating at the lateral canthus.
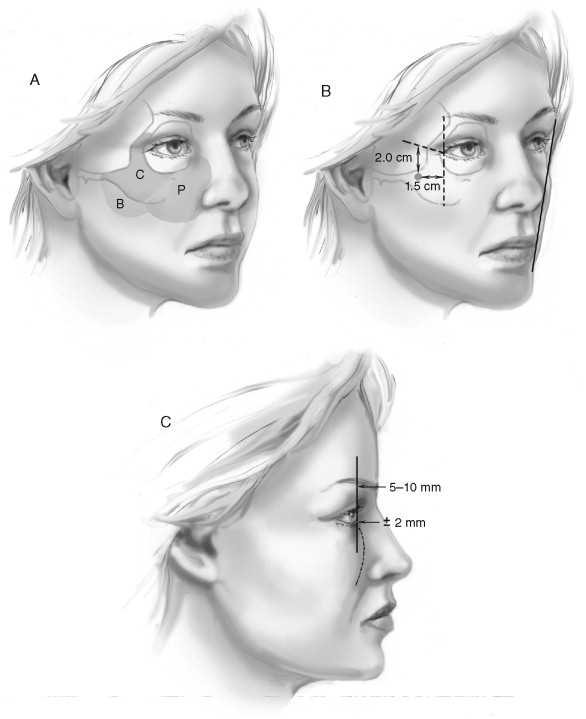
An imaginary line in three-quarter view from the lateral commissure to the lateral canthus allows identification of the most prominent aspect of the cheek and its inferior position relative to the lateral canthus. This location is also 15 to 20 mm inferior to the lateral canthus.
In profile the globe normally projects approximately 2 mm anterior to the lower lid, and from the lid inferiorly the midface is convex. The superior orbital rim projects 5 to 10 mm anteriorly to the anterior globe.
In frontal view the lateral-most projection of the malar eminence may also be related to the mandibular angle. Normally, a 7-degree angle is formed by the intersection of a malar eminence–mandibular angle tangent and a true vertical originating at the malar prominence, making the lateral projection of the malar eminence more lateral than the jaw angle.
Nose
Earlier in this chapter several general aspects of the nasal evaluation were discussed. Herein a more detailed anthropometric evaluation is presented. The nose is studied for form and symmetry. When deformities exist in the nose, their specific anatomic location—glabella, dorsum, tip, or alar bases—is noted ( Figure 1-5, A ).
| Vertical Proportions | Nasal Base | ||||
| Nose length/middle third height | N-Sn/G-Sn | 90% | Nasal tip width/alar width | Tip width/Al-Al | 75% |
| Dorsum length/middle third height | N-Pm/G-Sn | 80% | Tip length/nasal protrusion | Prn-C/Prn-Sn | 45% |
| Dorsum length/nose length | N-Pm/N-Sn | 90% | Columella length/nasal protrusion | C-Sn/Prn-Sn | 55% |
| Columella length/alar length | Sn-C/Ac-Prn | 35% | |||
| Horizontal Proportions | Nasal protrusion/alar width | Prn-Sn/Al-Al | 60% | ||
| Alar width/intercanthal width | Al-Al/En-En | 100% | Nasal protrusion/alar length | Prn-Sn/Ac-Prn | 60% |
| Nasal root width/alar width | Mf-Mf/Al-Al | 50% | Alar thickness | Ala | 5 mm |
| Nasal root width/intercanthal width | Mf-Mf/En-En | 50% | Columella thickness | Columella | 8 mm |
| Columella width/alar width | Columella/Al-Al | 25% |
Frontally the length of the nose (N-Sn) to that of the middle third of the face (G-Sn) is 90%. The dorsal nasal length (N-Prn) to midface (G-Sn) is 80%. Alar width (Al-Al)/intercanthal width (En-En) is 100%, and nasal root width (Mf-Mf)/alar width (Al-Al) is 50%.
Nasal tip width is 75% of alar width (Al-Al). Nasal tip defining points are approximately 10 mm apart.
In profile the nasofrontal angle is 135 degrees and the nasolabial is 100 degrees (see Figure 1-5, B ). Nasal protrusion (Sn-Prn) is 40% of nasal length (N-Sn), and nasal tip length (Prn-C) is 45% of nasal protrusion (Prn-Sn). Also, nasal protrusion (Prn-Sn) is 60% of both alar width (Al-Al) and alar length (Al-Prn).
Additional specific frontal and profile anthropometric relations are noted in the legend accompanying Figure 1-5 .
Perioral Area
The lips are extremely important in the overall esthetics of the face and are evaluated both in repose and during animation. At rest the symmetry of the lips relative to the face and the dentition is noted. If asymmetry exists, one must determine if the existing asymmetry is primarily the result of (1) an intrinsic lip deformity, as exists in many patients with clefts, (2) facial nerve dysfunction, or (3) an underlying dental-skeletal asymmetry. Each of these conditions requires different treatment considerations.
The upper teeth are normally exposed beneath the upper lip to 3 mm with the lips relaxed. There is less exposure in males than in females. An interlabial separation of up to 3 mm exists in repose. The width of the lips from commissure to commissure is normally approximately equal to the interpupillary distance (55 mm).
The lower lip has approximately 15% more vermilion exposed than the upper lip in repose. This ratio of exposed vermilion is more important than absolute values.
A frequent condition of the upper lip has been called the “gull-wing” upper lip. Normally the upper lip drape is such that its drape is coincident with a horizontal line from right to left commissures. The “gull-wing” lip is deficient vertically from point Sto laterally to the commissures.
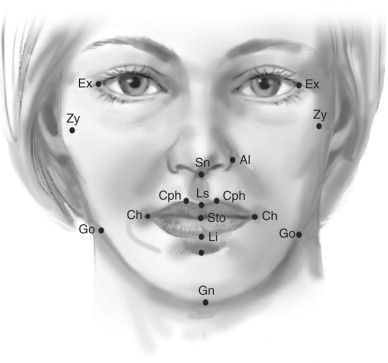
Several important anthropometric relationships of the lips are that the upper lip length (Sn-Sto) is 30% of the length or height of the lower third of the face (Sn-Gn), and the upper lip vermilion exposure (Ls-Sto) is 85% that of the lower lip (Sto-Li) vermilion exposure.
The normal width of the lips (Ch-Ch) is 55% of the width of the lower third of the face (Go-Go). The width of the mouth (Ch-Ch) is approximately half the bigonial width. Additional anthropometric relationships are noted in the legend to Figure 1-6 .
| Vertical Proportions | ||
| Upper lip/lower face | Sn-Sto/Sn-Gn | 30% |
| Lower lip/lower face | Sto-Sl/Sn-Gn | 25% |
| Chin/lower face | Sl-Gn/Sn-Gn | 45% |
| Lips | ||
| Upper lip/lower lip | Sn-Sto/Sto-Sl | 120% |
| Skin upper/lower lip | Sn-Ls/Sn-Sto | 70% |
| Skin lower/lower lip | Li-Sl/Sto-Sl | 60% |
| Vermilion upper/lower lip | Ls-Sto/Sto-Li | 85% |
| Horizontal Proportions | ||
| Mouth width/bigonial width | Ch-Ch/Go-Go | 55% |
| Mouth width/zygoma width | Ch-Ch/Zy-Zy | 40% |
| Mouth width/biocular width | Ch-Ch/Ex-Ex | 60% |
| Alar base width/mouth width | Al-Al/Ch-Ch | 65% |
| Philtrum width/mouth width | Chp-Chp/Ch-Ch | 20% |
| Columella width/philtrum width | Columella/Chp-Chp | 75% |
| Vertical/Horizontal Proportions | ||
| Upper lip height/mouth width | Sn-Sto/Ch-Ch | 40% |
| Lower face height/mouth width | Sn-Gn/Ch-Ch | 130% |
Ears
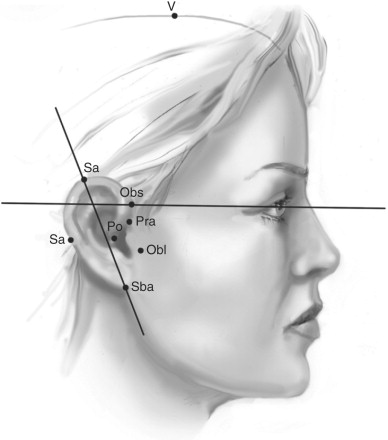
The ears are observed for symmetry, level, and projection. Any notable asymmetry is first recorded. Normal vertical level is present when the upper third of the ear projects above a horizontal line passed through the inner and outer canthi of the eyes. Finally, any abnormality in projection and any deformation or partial agenesis are noted ( Figure 1-7 ).
| Location | ||
| Vertical | V-Po | 130 mm |
| Horizontal | N-Obs | 115 mm |
| Lateral protrusion from malar bone | 25% | |
| Proportions | ||
| Width/length | Pra-Pa/Sa-Sba | 55% |
| Attachment length/vertical length | Obs-Obi/Sa-Sba | 85% |
| Angles | ||
| Medial long axis/horizontal | Sa-Sba/horizontal | 100% |
Cervicofacial Area
In this region, one sequentially evaluates both frontally and in profile the mandibular angle–inferior border definition, chin projection, soft tissue laxity, lipomatosis, and hyoid bone location.
Mandibular Angles and Inferior Borders.
The mandibular angles are assessed with regard to both their symmetry and their definition. The definition of the mandibular angles and inferior borders is an important consideration in neck esthetics, as this prominence (or lack thereof) defines the breaking point between the face and neck ( Figure 1-8 ). The neck relative to the mandible borders takes on a subtle hourglass appearance, with its superior aspect being well defined by the concavity immediately below the inferior mandibular borders. The soft tissues of the neck are normally closely adherent to the structures underlying them. The mandibular borders become less well defined when tissue laxity, lipomatosis, chin deficiency, and/or a low hyoid bone exist.
Chin-Neck Angle and Length.
The cervicomental angle is 100 degrees, and the neck-chin length is 50 mm (see Figure 1-8 ).
Chin Projection.
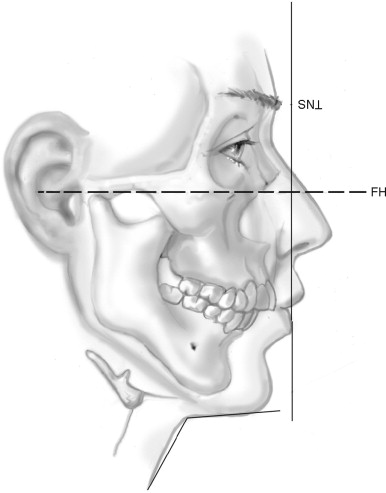
Chin projection can be most thoroughly evaluated cephalometrically as discussed next in this chapter. The chin normally is positioned approximately 4 mm behind SN perpendicular: a line drawn perpendicular to the Frankfort plane and passing through the SN. Neck-chin angle is normally 110 to 120 degrees, with the distance from the soft-tissue pogonion to neck-chin angle being approximately 50 mm. Frontally the width of the chin is assessed relative to the width of the midface (Zy-Zy) and the lower third of the face (Go-Go). Subjective assessment as to narrow, wide, or normal is made.
Lipomatosis.
Localized neck lipomatosis often exists independently of generalized body fat. The fat usually exists between the skin and the platysma muscle. This is readily assessed with gentle pinching of the skin.
Hyoid Bone Level.
The position of the hyoid bone is best assessed by grasping it gently between the thumb and index finger. Once the hyoid bone is grasped, its relation to the mandibular inferior border is noted. Normally the hyoid is no more than 20 mm below this border and just below the molar teeth (see Figure 1-8 ). When the hyoid bone is located more anterior and/or inferior than the norm, isolated soft-tissue cosmetic procedures in the neck will have limited results ( Box 1-1 ).
Clinical Evaluation of the Face
- 1.
Facial skin type (Fitzpatrick) _________
- 2.
Facial skin health (Glogau) _________
- 3.
General facial anthropometrics
- a.
Frontal face evaluation
-
Balance _________
-
Symmetry _________
-
Morphology _________
-
- b.
Profile evaluation
-
Upper third of the face
-
Middle third of the face
-
Lower third of the face
-
- a.
- 4.
Regional detailed evaluations
- a.
Periorbital area
- b.
Cheeks
- c.
Nose
- d.
Perioral area
- e.
Ears
- f.
Cervicofacial area
- a.
FACIAL SKIN AGE-RELATED CHANGES
Skin begins to undergo “aging” changes early in life that are primarily related to UV light exposure—more so than chronologic aging, smoking, genetics, or diet. However, current evidence reveals that these other factors do influence the rate and severity of skin aging. The actual rate of change is therefore highly variable, and so when I speak of age changes I do not consider them strictly chronologic.
Previously in this chapter the Glogau clinical skin damage (aging) classification method was discussed. Here I will discuss the underlying histologic-cellular changes that account for these observed clinical changes.
I will sequentially discuss the anatomic-histologic-cellular components of the various layers of the skin as follows: epidermis, dermis, vasculature, sebaceous apparatus, and subcutaneous fat. Reference to the normal skin anatomy and histology is helpful ( Figure 1-9 ). Of note when reviewing the facial skin is the variability of both the epidermis and dermis in different anatomic areas; note especially their differences in the forehead and neck. This variability is of importance in both their susceptibility to UV damage and skin rejuvenation approaches in different regions of the face.
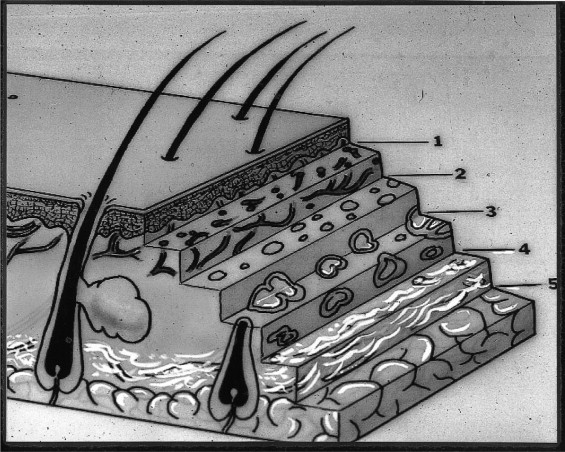
| RELATIVE SKIN DEPTHS (MICRONS) | ||
| 1. Epidermis | 125 a -250 b | |
| 2. Papillary dermis | 125-400 | |
| 3. Upper reticular dermis | 400-600 | |
| 4. Middle-lower reticular dermis | 600-1000 | |
| 5. Subcutaneous tissues | 1000-2000 | |
|
||
|
||
|
||
| Neck 150-25 | ||
Chronic UV exposure is the primary cause of the changes to be discussed that are attributed to aging skin. Accordingly, with cumulative sun exposure keratinocytes, melanocytes, and fibroblasts demonstrated markedly reduced replication rates and shorter life spans.
Changes in the Epidermis
With aging there occurs a thinning of the epidermis, with retraction or loss of the rete pegs evidenced by a flattening of the epidermal-dermal junction. One also notes an abnormal stratum corneum and loss of vertical polarity in the epidermis. These are in large part due to irreversible UV-induced DNA damage and a loss of proliferative potential of the keratinocytes. It has been reported that strictly photodamaged skin, as opposed to aged skin, exhibits a thickened epidermis.
The melanocytes that exist in the lower levels of the epidermis are injured secondary to UV-induced DNA damage, such that pigmentary changes in the skin occur that are clinically manifested as dyschromia or a variety of skin color changes and brown spots.
Changes in the Dermis
In viewing the normal skin as depicted in Figure 1-9 , the dermis is divided into the more superficial papillary dermis and the deeper reticular dermis. UV light or radiation, in the absence of proper UV skin protection, penetrates well into the dermis and is the primary determinant of dermal changes attributed to aging. A thinning of the dermis and a decrease in density of collagen and elastin fibers occur, along with, perhaps more important, a change from their normal parallel orientation into a random arrangement. There often occurs a slight thickening of individual elastic fibers. When this is excessive (i.e., large quantities of thickened bundles of elastic fibers are present), it is termed dermal elastosis
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


