An adenomatoid odontogenic tumor is an uncommon asymptomatic lesion that is often misdiagnosed as a dentigerous cyst. It originates from the odontogenic epithelium. Enucleation and curettage is the usual treatment of choice. Marsupialization may be attempted instead of extraction of the impacted tooth, since it provides an opportunity for tooth eruption. This case report is the first to report on the eruption of an impacted canine in an adenomatoid odontogenic tumor treated with combined orthodontics and marsupialization. The impacted canine erupted uneventfully, with no evidence of recurrence 3 years after the treatment.
Highlights
- •
Adenomatoid odontogenic tumor (AOT) is an uncommon asymptomatic lesion that is often misdiagnosed as a dentigerous cyst.
- •
The clinical and radiologic findings of the AOT mimic a dentigerous cyst.
- •
Surgical enucleation and curettage is the standard treatment for AOT.
- •
Marsupialization was selected for treatment of our patient. In this way, the functional and esthetic features were ensured.
An adenomatoid odontogenic tumor is a relatively rare benign lesion. Although many terms have been used to describe this disease, the World Health Organization named it “adenomatoid odontogenic tumor” in 1971. It is most frequently observed in the anterior maxilla, followed by the anterior mandible. Although there are some reported differences, the female-to-male ratio is about 2:1 in all age groups and for all variants. Generally, the disease occurs in the second decade of life. Clinically, an adenomatoid odontogenic tumor resembles a dentigerous cyst or an ameloblastoma. But unlike an ameloblastoma, an adenomatoid odontogenic tumor is a benign, painless, noninvasive, slow-growing tumor that does not infiltrate bone. It is completely radiolucent and mimics a dentigerous cyst in growth pattern and appearance. However, it often appears to envelop both the crown and roots of a tooth, unlike a dentigerous cyst, which does not envelop the roots. A histopathologic examination is the most important assessment in the differential diagnosis.
Because of the slow growth and asymptomatic nature of the lesion, patients are usually diagnosed incidentally. An adenomatoid odontogenic tumor is generally smaller than 3 cm, with a solid or cystic structure, but rarely can grow to a large size. Three types of adenomatoid odontogenic tumors have been described—follicular, extrafollicular, and peripheral—with the follicular type being the most common.
Surgical enucleation and curettage is the standard treatment of choice because of the encapsulated, benign, noninvasive, and nonaggressive characteristics of the lesion. During this procedure, the impacted tooth is usually excised with the lesion. The reported results for almost all adenomatoid odontogenic tumors treated with enucleation are good, and recurrence is rare. This article presents a patient with an impacted permanent mandibular canine, which was diagnosed as an adenomatoid odontogenic tumor after histopathologic examination, and was treated with marsupialization.
Case report
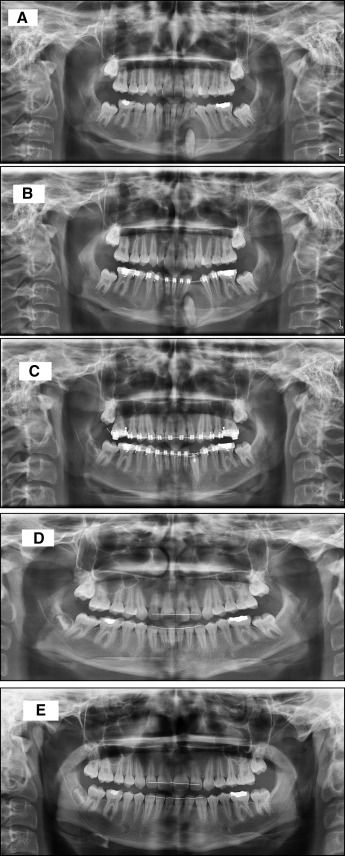
A 12-year-old girl consulted the Department of Orthodontics at Selcuk University in Turkey with the chief complaint of an unesthetic dental appearance. Clinically, she had a well-balanced facial profile and Class II molar and canine relationships on both sides, with maxillary anterior crowding, increased overbite, and mandibular dental midline deviation ( Fig 1 ). She had a mandibular left deciduous canine and painless swelling in the mandibular left vestibule ( Fig 2 , A ). Cephalometric and panoramic radiographs and dental casts were obtained. Radiologically, her permanent canine was an impacted, well-circumscribed radiolucency that looked like a cystic lesion that started from the middle of the root and surrounded the crown completely with a well-defined corticated border. There was migration of the neighboring teeth. The swelling extended from the left lateral incisor to the left premolar both buccally and lingually. On palpation, its consistency was firm. Based on the clinical and radiographic findings, an adenomatoid odontogenic tumor or a dentigerous cyst was considered the primary diagnosis.

In consultation with the Department of Oral and Maxillofacial Surgery at our university, we attempted to allow the tooth to erupt with marsupialization. The mandibular deciduous left canine was extracted under an inferior alveolar nerve block. Then, a mucoperiosteal flap was elevated, the bone window was extended, and the upper part of the lesion was excised from the bone window border. A biopsy sample was taken and sent for histopathologic examination. After the wound was irrigated with saline solution, the crown of the impacted canine was observed in the cavity. The cavity was filled with antibiotic gauze, and then the flap was sutured in the primary position. The patient was recalled to irrigate the cavity with saline solution and to replace the antibiotic gauze in the socket every 2 days. After 1 week, an impression model was obtained to design an obturator for a cavity, which the patient wore for nearly 4 months. Her parents were taught to clean the cavity every day with saline solution and an injector.
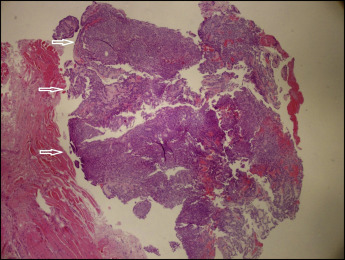
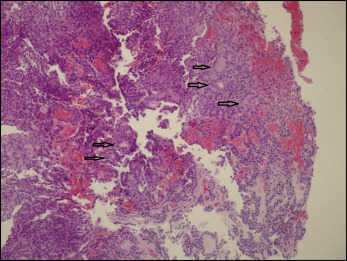
The histopathologic examination of the biopsy showed an adenomatoid odontogenic tumor. Well-circumscribed proliferation of the duct-like epithelium, which had a rosette formation with calcification, was observed in the center. Columnar epithelial cells with basal nuclei and clear cytoplasm resembled preameloblasts. Eosinophilic fibrillar material was present between the tumor cells and in the duct-like structures. Rare mitoses, no necrosis, and no epithelial atypia were detected ( Figs 3 and 4 ).