Introduction
The aim of this systematic review was to compare the effectiveness of orthodontic miniscrew implants—temporary intraoral skeletal anchorage devices (TISADs)—in anchorage reinforcement during en-masse retraction in relation to conventional methods of anchorage.
Methods
A search of PubMed, Embase, Cochrane Central Register of Controlled Trials, and Web of Science was performed. The keywords were orthodontic, mini-implants, miniscrews, miniplates, and temporary anchorage device. Relevant articles were assessed for quality according to Cochrane guidelines and the data extracted for statistical analysis. A meta-analysis of raw mean differences concerning anchorage loss, tipping of molars, retraction of incisors, tipping of incisors, and treatment duration was carried out.
Results
Initially, we retrieved 10,038 articles. The selection process finally resulted in 14 articles including 616 patients (451 female, 165 male) for detailed analysis. Quality of the included studies was assessed as moderate. Meta-analysis showed that use of TISADs facilitates better anchorage reinforcement compared with conventional methods. On average, TISADs enabled 1.86 mm more anchorage preservation than did conventional methods ( P <0.001).
Conclusions
The results of the meta-analysis showed that TISADs are more effective than conventional methods of anchorage reinforcement. The average difference of 2 mm seems not only statistically but also clinically significant. However, the results should be interpreted with caution because of the moderate quality of the included studies. More high-quality studies on this issue are necessary to enable drawing more reliable conclusions.
Highlights
- •
Effectiveness of temporary intraoral skeletal anchorage devices (TISADs) was assessed.
- •
Fourteen articles representing 616 patients with TISADs were selected for meta-analysis.
- •
Quality of the included studies was moderate.
- •
TISADs were more effective than conventional methods of anchorage reinforcement.
- •
The average difference of 2 mm was statistically and clinically significant.
The resistance to undesirable maxillary mesial molar movement while closing maxillary arch spaces after extraction of the first or second premolars is a key element of anchorage control and is obviously crucial for optimal treatment results. Successful treatment of an adult with a full Class II malocclusion and maxillary dentoalveolar protrusion necessitating closure of the extraction spaces entirely from the front (by retraction of anterior teeth only) requires maximum anchorage achievable with various methods.
Extraoral appliances, although efficient in anchorage control, highly depend on the patient’s compliance and are therefore considered a fallible form of anchorage control with variable levels of outcome. Moreover, they have been associated with isolated cases of facial injury. On the other hand, the effectiveness of intraoral appliances—eg, a Nance holding arch or transpalatal bar—has been questioned with prospective research alluding to limited benefits during active appliance therapy.
Orthodontic implants or temporary intraoral skeletal anchorage devices (TISADs) are a compliance-free alternative to more traditional forms of anchorage. They are not attached directly to the teeth, unlike other methods of anchorage reinforcement. TISADs are regarded as simple to place and have reported survival rates ranging from 80% to 94% and have therefore been advocated as the potential method of choice when anchorage reinforcement is necessary during treatment. However, there is some disagreement about the precise effects of TISADs during space closure; several recent studies have demonstrated significant anchorage losses, whereas others found the opposite effect. Moreover, there is conflicting evidence relating to their effectiveness vs alternative approaches to anchorage supplementation.
The aim of this systematic review and meta-analysis was to compare the effectiveness of TISADs and conventional anchorage augmentation during space closure by retraction of anterior teeth.
Material and methods
We performed this study according to PRISMA guidelines, and the main research question was defined in PICO format ( Table I ).
| Population | Subjects requiring absolute anchorage in maxillary arch |
|---|---|
| Intervention | Retraction of anterior teeth with TISADs |
| Comparison | Retraction of anterior teeth with conventional anchorage |
| Outcome | Anchorage loss, change in angulation of maxillary molars, amount of incisors’ retraction, change in angulation of maxillary incisors, and treatment duration |
Eligibility criteria
- 1.
Study design: randomized controlled trials (RCTs) and controlled clinical trials (CCTs).
- 2.
Participants: orthodontic subjects requiring extraction of the maxillary first premolars and closure of the spaces without anchorage loss.
- 3.
Interventions: study group, anchorage reinforcement with TISADs; control group, conventional anchorage reinforcement.
- 4.
Exclusion criteria: language other than English, animal studies, case reports, case-series reports, literature reviews, lack of control group or fewer than 10 subjects in the study group, patients not treated with sliding mechanics, or comparison of anchorage loss after retraction of canines only.
- 5.
Outcome measures: the primary outcome was anchorage loss defined as mesial movement of the maxillary first molars. Secondary outcomes were change in the angulation of the maxillary molars, amount of incisor retraction, change in the angulation of the maxillary incisors, and treatment duration.
Search strategy, study selection, and information sources
The search strategy of the electronic databases, PubMed, EMBASE, Cochrane Central Register of Controlled Trials, and Web of Science (1990 to March 2016) is shown in Table II . Based on information from the titles and abstracts, relevant articles meeting the following inclusion criteria were selected: written in English, research on humans treated with extraction of the maxillary first premolars and retraction of all 6 anterior teeth with absolute anchorage, sliding mechanics used, and more than 10 subjects in the study group. Electronic searching was supplemented with review of the bibliography in each identified article. The following journals were manually screened: European Journal of Orthodontics , Journal of Orthodontics , Journal of Clinical Orthodontics , Seminars in Orthodontics , American Journal of Orthodontics & Dentofacial Orthopedics , and Angle Orthodontist . The literature search, assessment of relevance, risk of bias analysis, and data extraction were performed independently by 2 authors (J.A.S. and J.Ł.). All authors discussed disagreements until consensus was reached.
| Database | Key words | Limits |
|---|---|---|
| PubMed | orthodontics and implant or micro-implant or microimplant or mini-screw or miniscrew or screw implant or temporary anchorage device or palatal implant or midpalatal implant or mini-plate or miniplate or en masse retraction | English language, studies on humans, 1990 to March 2016 |
| EMBASE | orthodontics and implant or micro-implant or microimplant or mini-screw or miniscrew or screw implant or temporary anchorage device or palatal implant or midpalatal implant or mini-plate or miniplate or en masse retraction | English language, studies on humans, 1990 to March 2016 |
| Cochrane Central Register of Controlled Trials | orthodontics and implant or micro-implant or microimplant or mini-screw or miniscrew or screw implant or temporary anchorage device or palatal implant or midpalatal implant or mini-plate or miniplate or en masse retraction | English language, studies on humans, 1990 to March 2016 |
| Web of Science | orthodontics and implant or micro-implant or microimplant or mini-screw or miniscrew or screw implant or temporary anchorage device or palatal implant or midpalatal implant or mini-plate or miniplate or en masse retraction | English language, studies on humans, 1990 to March 2016 |
Data extraction
The following data were extracted from the included studies: year of publication, sample size, age of the patients at the beginning of the treatment, types of appliances used for anchorage reinforcement, types and dimensions of the TISADs, amounts of mesial molar movement and tipping, amounts of incisor retraction and tipping, and treatment duration.
Risk of bias in individual studies
The Cochrane Collaboration tool for assessing risk of bias in randomized controlled trials was applied using the following criteria: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of assessors, incomplete outcome data, selective reporting of outcomes, and other potential sources of bias. The quality of the CCTs was assessed according to a modified Newcastle-Ottawa Scale ( Appendix ) comprising 3 sections.
- 1.
“Selection,” evaluating case definition, representativeness of cases, control selection, and definition of controls. Each aspect was assigned 1 mark, giving 4 marks in total.
- 2.
“Comparability,” appraising extraction patterns in the maxilla and the mandible; therefore, 2 marks could be obtained in this section.
- 3.
“Outcome assessment,” evaluating outcome measures, treatment changes, and blinding of assessors, giving 3 marks in total.
Summary measures and approach to synthesis
Random-effects meta-analysis of the mean differences in mesial movement of the molars, tipping of the molars, retraction of the incisors, tipping of the incisors, and treatment duration was carried out. Randomized and controlled clinical studies were statistically evaluated both jointly and separately with subgroup analysis and significance established at P <0.05. Results of the analyses are presented graphically with forest plots after comparisons of study designs, methodologies, participants, and types of anchorage to judge the clinical heterogeneity of the studies. The Cochrane Q test and I 2 statistics enabled evaluation of statistical heterogeneity of the collected data. All calculations were carried out with STATISTICA Medical Bundle software (version 3.0; StatSoft Polska, Krakow, Poland).
Additional analysis
Sensitivity analysis was performed by drawing sensitivity plots to define the influence of specific studies on the total calculated effect. Funnel plot analysis involving Begg and Mazumdar and Egger asymmetry tests allowed assessment of publication bias.
Results
Retrieved studies and data extraction
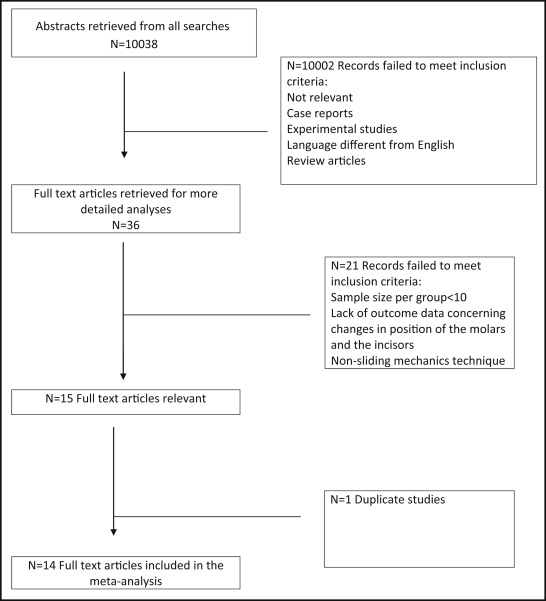
The PRISMA diagram depicting the flow of the 10,038 initially retrieved articles is presented in Figure 1 . Review of the abstracts excluded 10,002 of them, leaving 36 full-text articles. Subsequently, 21 studies were found to be ineligible for further analysis because of insufficient sample size or lack of relevant outcome data. Two of the retrieved 15 eligible studies were based on the same sample of patients; therefore, only 1 was used in this systematic review. Eventually, we obtained 7 RCTs and 7 CCTs, giving a total of 14 studies. A summary of the data extracted from the articles is shown in Table III , and the demographic structure of the pooled patient sample is given in Table IV . In total, 616 patients were included: 451 female and 165 male. Three hundred three patients were treated using TISADs (mini-implants, miniplates, or miniscrews). That group included 231 female and 72 male patients. The control group comprised 313 patients, 220 female and 93 male, treated with conventional anchorage reinforcement. The mean ages of the patients at the beginning of treatment were 19.43 years in the TISAD group and 18.21 years in the conventional anchorage group.
| Study | Diameter/length (mm) of TISAD | Magnitude of force (G) | Mesial molar movement-anchorage loss (mm) ∗ | Tipping of molars (°) ∗ | Incisor distalization (mm) ∗ | Incisor tipping (°) ∗ | Treatment duration (mo) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Miniscrew | Miniplate | Hg/TPA | TISAD/Hg | TISAD/Hg | TISAD/Hg | Miniscrew | Miniplate | Hg/TPA | ||||||
| RCTs | ||||||||||||||
| Benson et al, 2007 | NR/6 mm | 450 | 1.5 | 3 | NR/NR | −2.1/−0.7 | NR/NR | NR | NR | |||||
| Lai et al, 2008 | Various | 300-350 | 1.3 | 1.4 | 2.5 | NR/NR | −6.9/−7.3/−5.5 | NR/NR/NR | 27.1 ± 4.2 | 31.4 ± 4.7 | 33.6 ± 7.2 | |||
| Upadhyay et al, 2008 | 1.3/8 | 300-350 | −0.78 | 3.22 | NR/NR | −7.22/−6.33 | −13.11/−16.83 | NR | NR | |||||
| Feldmann and Bondemark, 2008 | 1.3/8 mm | NR | PI 0.1 |
Hg 2.0 |
On −0.2 |
Hg 0.8 |
On −3.9 |
Hg −4.8 |
On −1.7 |
Hg −1.9 |
NR | NR | ||
| On −0.1 |
TPA 1.0 |
PI 0.7 |
TPA 0.7 |
PI −4.7 |
TPA −3.3 |
PI −3.0 |
TPA −1.1 |
NR | NR | |||||
| Liu et al, 2009 | 1.2/8 mm | NR | −0.06 | 1.47 | NR/NR | −7.03/−4.76 | −13.53/−12.03 | 20.65 ± 5.06 | 26.88 ± 6.54 | |||||
| Lee and Kim, 2011 | 1.6/8 mm | NR | 0.24 | 2.2 | 0.49/−0.25 | −9.45/−7.10 | −16.20/−19.13 | 24.95 ± 4.55 | 28.00 ± 8.37 | |||||
| Koyama et al, 2011 | 1.6/8 mm | 200 | 0.1 | 2.1 | NR/NR | −6.2/−7.0 | −10.3/−11.1 | NR | NR | |||||
| Al-Sibae and Hajeer, 2013 | 1.6/7 mm | 300 | −0.75 | 1.76 | NR/NR | −5.92/−4.79 | −5.03/−7.94 | 12.9 ± NR | 16.97 ± NR | |||||
| Victor et al, 2014 | 1.3/8 mm | 150 | NR | NR | −0.88/3.38 | NR | −5.8/−5.8 | NR | NR | |||||
| Sandler et al, 2014 | 1.6/8 mm | 100 | 0.99 | Na 2.09 | NR | NR | NR | 26.83 (8.5-45.16) | Hg 28.01 (17.46-38.51) | |||||
| Hg 1.99 | TPA 27.43 (15.03-39.83) | |||||||||||||
| CCTs | ||||||||||||||
| Park et al, 2008 | 1.3/8 mm | 150 | 0.26 | 1.71 | −1.40/−0.17 | −8.58/−7.47 | −14.39/−19.29 | 25.6 ± 5.5 | 28.6 ± 4.2 | |||||
| Upadhyay et al, 2008 | 1.3/8 | 300-350 | −0.55 | 1.95 | −0.13/3.7 | −0.9/0.37 | −11.27/−10.83 | NR | NR | |||||
| Yao et al, 2008 | Various | 300-350 | 0.88 | 2.07 | NR/NR | −8.17/−6.73 | −13.56/−9.59 | 29.81 ± 6.41 | 32.29 ± 6.46 | |||||
| Kuroda et al, 2007 | 1.3/8 | NR | 0.7 | 3 | NR/NR | −9.3/−6.3 | −20.3/−14.0 | NR | NR | |||||
| Lee and Kim, 2011 | 1.6/8 mm | NR | 0.24 | 2.2 | 0.49/−0.25 | −9.45/−7.10 | −16.20/−19.13 | 24.95 ± 4.55 | 28.00 ± 8.37 | |||||
| Koyama et al, 2011 | 1.6/8 mm | 200 | 0.1 | 2.1 | NR/NR | −6.2/−7.0 | −10.3/−11.1 | NR | NR | |||||
∗ For linear measurements, + indicates mesial movement and–distal movement; for angular measurements, + indicates mesial tipping and − distal tipping.
| Study | TISAD | Conventional anchorage | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | Male | n | % female | Age at start of treatment (y) | Success rate (%) | Female | Male | n | % female | Age at start of treatment (y) | |
| Benson et al, 2007 | 20 | 6 | 26 | 76.92 | 15.70 | 75.00 | 18 | 7 | 25 | 72.00 | 14.80 |
| Park et al, 2008 | 14 | 2 | 16 | 87.50 | 22.50 | 87.00 | 11 | 3 | 14 | 78.57 | 22.90 |
| Upadhyay et al, 2008 | 10 | 5 | 15 | 66.67 | NR | 87.00 | 11 | 4 | 15 | 73.33 | NR |
| Lai et al, 2008 | 21 | 3 | 24 | 87.50 | 24.73 | NR | 16 | 0 | 16 | 100.00 | 21.70 |
| Yao et al, 2008 | 23 | 2 | 25 | 92.00 | 24.72 | NR | 20 | 2 | 22 | 90.91 | 22.23 |
| Upadhyay et al, 2008 | 20 | 0 | 20 | 100.00 | 17.60 | 93.00 | 20 | 0 | 20 | 100.00 | 17.30 |
| Feldmann and Bondemark, 2008 | 30 | 30 | 60 | 50.00 | 14.30 | 88.37 | 30 | 30 | 60 | 50.00 | 14.20 |
| Kuroda et al, 2007 | 11 | 0 | 11 | 100.00 | 18.50 | NR | 11 | 0 | 11 | 100.00 | 21.80 |
| Liu et al, 2009 | 14 | 3 | 17 | 82.35 | 19.71 | 88.00 | 14 | 3 | 17 | 82.35 | 21.65 |
| Lee and Kim, 2011 | 20 | 0 | 20 | 100.00 | 24.64 | NR | 20 | 0 | 20 | 100.00 | 22.16 |
| Koyama et al, 2011 | 13 | 1 | 14 | 92.86 | 24.80 | 86.00 | 12 | 2 | 14 | 85.71 | 25.00 |
| Al-Sibae and Hajeer, 2013 | 19 | 9 | 28 | 67.86 | 23.02 | 95.00 | 16 | 12 | 28 | 57.14 | 20.46 |
| Victor et al, 2014 | NR | NR | 10 ∗ | NR | NR | NR | NR | NR | 10 ∗ | NR | NR |
| Sandler et al, 2014 | 16 | 11 | 27 | 59.26 | 14.15 | NR | 21 | 30 | 51 | 41.18 | 14.26 |
| Summary | 231 | 72 | 303 | 76.24 | 19.43 | 87.60 | 220 | 93 | 313 | 70.29 | 18.21 |
| Incisor retraction | 215 | 61 | 276 | 77.90 | 19.97 | 87.60 | 199 | 63 | 262 | 75.95 | 19.02 |
| Incisor tipping | 174 | 52 | 226 | 76.99 | 19.96 | 89.52 | 165 | 56 | 221 | 74.66 | 19.33 |
| Mesial molar movement | 231 | 72 | 303 | 76.24 | 19.43 | 87.60 | 220 | 93 | 313 | 70.29 | 18.21 |
| Molar tipping | 74 | 37 | 111 | 66.67 | 17.82 | 87.90 | 72 | 37 | 109 | 66.06 | 17.19 |
| Treatment duration | 92 | 10 | 102 | 90.20 | 23.52 | 87.52 | 81 | 8 | 89 | 91.01 | 22.11 |
Risk of bias within studies
The assessment of the risk of bias in the RCTs is presented in Table V and summarized in Figure 2 . We assessed the risk of bias from randomization as low in the studies by Feldmann and Bondemark, Benson et al, Upadhyay et al, Al-Sibae and Hajeer, and Sandler et al, who presented precisely described, rigorous randomization methods (computer-generated random numbers or external randomization center). Due to lack of information about the randomization process, we assessed the studies by Liu et al and Victor et al as having an unclear risk of bias. For allocation concealment, the studies by Feldmann and Bondemark, Upadhyay et al, Al-Sibae and Hajeer, and Sandler et al were evaluated as having a low risk of bias, since opaque sealed envelopes were used in this respect. Because the type of anchorage reinforcement becomes obvious during its application, blinding of participants and personnel to the treatment method was not feasible. Thus, risk of bias had to be graded as high in all included studies. On the other hand, this shortcoming was partly overcome by blinding of the outcome assessment. Four studies, those of Benson et al, Upadhyay et al, Al-Sibae and Hajeer, and Sandler et al precisely described the blinding of assessors or the introduction of a person not involved in the study and unaware of its purpose. The other authors skipped that information; thus, the risk of bias remained unclear. All studies were assessed as having a low risk of bias from lack of complete data, selective reporting, or other threats to validity.


