A 22-year-old woman came with a unilateral missing mandibular first molar and buccal crossbite. The open space was closed by protraction of the mandibular left second molar and uprighting and protraction of the horizontally impacted third molar using temporary skeletal anchorage devices, and her buccal crossbite was corrected with modified palatal and lingual appliances. The total active treatment time was 36 months. Posttreatment records after 9 months showed excellent results with a stable occlusion.
Highlights
- •
We uprighted a horizontally impacted third molar with orthodontics.
- •
The mandibular second and third molars were protracted into the missing first molar space.
- •
We corrected a buccal crossbite with modified palatal and lingual appliances.
The development of temporary skeletal anchorage devices (TSADs) has opened a new paradigm in modern orthodontics, offering treatment options for many difficult conditions that were untreatable with conventional methods. Absolute anchorage can be achieved with TSADs because the anchorage device is fixed in bone, eliminating anchorage loss that caused dental shifting or tilting, side-effects commonly seen with conventional intraoral anchorage appliances.
Edentulous spaces caused by missing mandibular first molars are a common problem for clinicians. Various methods have been used to replace or remove this condition: dental implants, dental bridges, and space closure with orthodontics. TSADs allow maximum anchorage for molar protraction to close these spaces.
Likewise, a posterior crossbite is a common malocclusion in deciduous and mixed dentitions. It has been claimed that stimuli through the teeth and musculature are what maintain alveolar bone architecture and shape. Changes in the stimuli acting on the bone cause bone remodeling. If a posterior crossbite is left untreated, it can lead to skeletal deformation, so it is imperative that tooth position and musculature be corrected as soon as possible to prevent complications.
The primary feature of posterior crossbite is at least 1 tooth in the maxillary arch ectopically positioned buccally or lingually with respect to the corresponding mandibular tooth or teeth. Posterior crossbite can be bilateral or unilateral. It also has been reported that in children with unilateral posterior crossbite, the activity of the temporal and masseter muscles can be disturbed, and that adolescent patients with posterior crossbite have an increased risk of developing temporomandibular disorders. Better prognosis and simple correction of posterior crossbites are possible when patients are in the deciduous and mixed dentitions; therefore, a posterior crossbites should be corrected early to eliminate future functional and skeletal problems. If these patients are treated as adults, we predict more side effects and prolonged treatment times.
In this case report, we present a woman with posterior crossbites and a missing mandibular left first molar. Her buccal crossbite was corrected successfully with modified palatal and lingual appliances, and the lingual crossbite was improved with wire expansion. Her missing mandibular left first molar space was closed by protraction of the left second molar and uprighting and protraction of the third molar using TSADs and a mandibular lingual holding arch with an extension arm. See Supplemental Materials for a short video presentation about this study.
Diagnosis and etiology
A 22-year-old woman was referred to a private office for an evaluation of orthodontic treatment. Her chief complaint was protrusion of her maxillary anterior teeth. She had a dolichofacial pattern and a Class II appearance. A hyperactive mentalis muscle with lip strain was seen when she attempted to close her lips. She also had decreased lower anterior facial height. There was no significant facial asymmetry.
Intraorally, she had proclined maxillary incisors with overjet of 8.5 mm and overbite of 70%. She showed an end-on Class II molar relationship on her right side, but the left-side molar occlusion was not classified because of her missing mandibular left first molar. She had moderate crowding in her maxillary arch and a deep curve of Spee in her mandibular arch. In addition, she had a slight lingual crossbite on her maxillary right first molar and a buccal crossbite on the maxillary left second molar. The occlusal anatomy and contour of the maxillary first molar crowns were poor. When her mandible was guided into centric relation, a functional shift was detected because of her posterior crossbites. Compared with her facial midline, her maxillary dental midline was coincident, but her mandibular dental midline was deviated 1.5 mm to the right ( Figs 1 and 2 ).


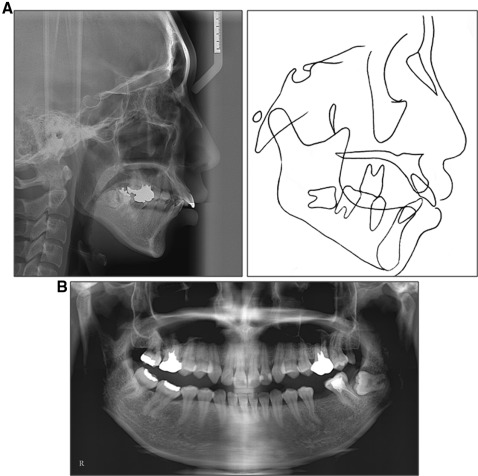
A panoramic radiograph showed slightly different right and left condylar heads, but during the temporomandibular joint evaluation, the patient did not report any muscle or joint pain or other symptoms typically associated with temporomandibular disease. She was missing her right third molars. She had a maxillary left third molar (mirocrodontia) and a horizontally impacted mandibular left third molar. The root apices of the mandibular third molar were close to the inferior alveolar nerve. The mandibular left second premolar had a dilacerated root, and the mandibular right molars showed mesial tilting. Her maxillary first molars had been restored with crowns after endodontic treatment.
The lateral cephalometric analysis indicated a skeletal Class II pattern (ANB, 5.5°) with a hyperdivergent growth pattern (SN-MP, 40.0°). The maxillary and mandibular incisors were proclined (U1-SN, 112.0°; IMPA, 98.0°) ( Fig 3 ; Table ).
| Measurement | Norm | Pretreatment | Posttreatment | 9-month retention |
|---|---|---|---|---|
| SNA (°) | 82.0 | 77.5 | 77.0 | 77.5 |
| SNB (°) | 80.0 | 72.0 | 71.0 | 71.5 |
| ANB (°) | 2.0 | 5.5 | 5.0 | 5.0 |
| Wits (mm) | −1.0 | 3.5 | −1.5 | −1.0 |
| SN-MP (°) | 32.0 | 40.0 | 41.0 | 41.0 |
| FH-MP (°) | 24.0 | 34.0 | 35.0 | 35.5 |
| LFH (ANS-Me/N-Me) (%) | 55.0 | 51.3 | 55.0 | 55.5 |
| U1-SN (°) | 104.0 | 112.0 | 94.0 | 93.5 |
| IMPA (°) | 90.0 | 98.0 | 100.0 | 100.0 |
| U1/L1 (°) | 131.0 | 107.0 | 124.0 | 124.5 |
| Upper lip (mm) | −4.0 | 3.0 | 0.0 | 0.0 |
| Lower lip (mm) | −2.0 | 4.0 | 1.5 | 1.5 |
Treatment objectives and plan
The following treatment objectives were established: (1) relieve crowding in the maxillary arch and close the space in the mandibular arch, (2) correct the posterior crossbites, (3) establish Class I canine and Class I (or Class II) molar relationships, (4) obtain normal overjet and overbite, (5) level the curve of Spee, (6) improve the deviation when she opened her mouth and correct the dental midline, (7) obtain a stable occlusal relationship, and (8) improve facial and dental esthetics by establishing an esthetic smile.
With TSADs, distal movement of maxillary anterior teeth or mesial movement of mandibular posterior teeth would be possible without anchorage loss. Because the patient wanted to retract her upper lip as much as possible, the plan was to extract her maxillary first premolars. To camouflage the skeletal Class II pattern without a dental implant restoration (as per the patient’s request), her mandibular second premolars were not extracted even though her mandibular incisors were proclined. The treatment plan was to protract her mandibular left second molar as a substitute for the first molar and protract her impacted third molar to replace the second molar after surgical exposure and uprighting. To correct the lingual crossbite on the maxillary right first molar, wire expansion was planned. To correct the buccal crossbite on the maxillary left second molar, modified palatal and lingual appliances were planned to be used.
Treatment objectives and plan
The following treatment objectives were established: (1) relieve crowding in the maxillary arch and close the space in the mandibular arch, (2) correct the posterior crossbites, (3) establish Class I canine and Class I (or Class II) molar relationships, (4) obtain normal overjet and overbite, (5) level the curve of Spee, (6) improve the deviation when she opened her mouth and correct the dental midline, (7) obtain a stable occlusal relationship, and (8) improve facial and dental esthetics by establishing an esthetic smile.
With TSADs, distal movement of maxillary anterior teeth or mesial movement of mandibular posterior teeth would be possible without anchorage loss. Because the patient wanted to retract her upper lip as much as possible, the plan was to extract her maxillary first premolars. To camouflage the skeletal Class II pattern without a dental implant restoration (as per the patient’s request), her mandibular second premolars were not extracted even though her mandibular incisors were proclined. The treatment plan was to protract her mandibular left second molar as a substitute for the first molar and protract her impacted third molar to replace the second molar after surgical exposure and uprighting. To correct the lingual crossbite on the maxillary right first molar, wire expansion was planned. To correct the buccal crossbite on the maxillary left second molar, modified palatal and lingual appliances were planned to be used.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


