Introduction
The purpose of this study was to assess the anatomic structure of the buccal alveolar bone in the infrazygomatic crest region with cone-beam computed tomography to locate safe zones for miniscrews in maxillary dentition distalization.
Methods
The buccal alveolar bone was analyzed in 3 regions of 60 patients: between the maxillary second premolar and first molar (U5-U6), between the mesiodistal roots of the first molar (U6), and between the maxillary first and second molars (U6-U7). Alveolar bone thickness at the buccal side of the roots and the interradicular space at the buccal side of the roots were measured at the planes of 5, 7, 9, and 11 mm apically from the alveolar crest to the maxillary sinus floor. The buccal bone height was measured from the alveolar crest edge to the sinus floor.
Results
The buccal alveolar bone was thicker in the U6-U7 region than in the U6 and U5-U6 regions. The buccal alveolar bone thickness tended to get thicker from the alveolar crest to the sinus floor. The thickest buccal alveolar bone of 4.07 mm was observed at the plane of 11 mm of the U6-U7 region. The percentages for the height of bone from the crest edge to the sinus floor were smaller than 10 mm at the regions of U5-U6, U6, and U6-U7: 38%, 52%, and 43%, respectively. The interradicular space was smallest in the U6 region and largest in the U5-U6 region.
Conclusions
The results of this study suggest that the U6-U7 region is the most ideal safe zone for placing miniscrews in the buccal alveolar bone in the infrazygomatic crest region for maxillary dentition distalization.
Highlights
- •
Buccal alveolar bone was thicker in the U6-U7 region than in the U6 and U5-U6 regions.
- •
Buccal alveolar bone thickness increased from the alveolar crest to the sinus floor.
- •
Interradicular space was greatest in the U5-U6 region and least in the U6 region.
- •
For miniscrew placement in the buccal alveolar bone in the infrazygomatic crest, U6-U7 is preferred.
Anchorage is the most important factor that affects the treatment plan and the orthodontic treatment result. Recently, different kinds of skeletal anchorage have attracted the attention of orthodontists. Miniscrews originally used for bone fixation have been used widely as auxiliary anchorage devices for tooth movement without a great compliance requirement for orthodontic patients.
Treatment of Class II malocclusion frequently requires distalization of the maxillary molars into a Class I relationship. However, when the first molars are moved distally after the eruption of the second molars, they tend to move slowly, and anchorage loss happens frequently. Hence, distalization of the maxilliary molars is relatively more difficult than other types of tooth movement. A few reports have demonstrated that the molars can be distalized successfully with virtually no anchorage loss. Headgear that has been frequently used to distalize the maxilliary molars in adolescent patients is seldom used for adults because of esthetic and compliance concerns. Skeletal anchorage has been proposed for this situation. Sugawara et al proposed maxillary dentition distalization by using titanium anchor plates, and Kook et al used palatal anchorage plates for distalization of the maxillary dentition. The use of miniscrews, which offer more simple and stable force systems, has gradually become popular and reliable.
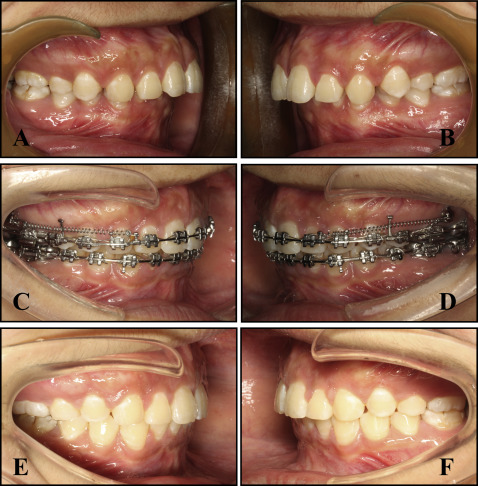
The miniscrew has been widely used in the clinic because of its advantages, including smaller size, simpler surgical placement, shorter (or even no) waiting period, easier removal after treatment, and lower cost. A new method for distalization of the entire maxillary dentition is using miniscrews implanted in the infrazygomatic crest, as proposed by Liou et al and Lin and Liou. Liou et al suggested that miniscrew insertion sites in the infrazygomatic crest of adults are 14 to 16 mm above the maxillary occlusal plane and at an angle of 55° to 70° to the maxillary occlusal plane. In recent years, our department has widely used miniscrews as anchorage for the distal movement of the maxillary dentition and achieved excellent clinical outcomes ( Fig 1 ). The purposes of this study were to study the thickness and height of the alveolar bone in the buccal region of posterior roots via the cone-beam computed tomography (CBCT) technique and to provide guidelines for choosing the appropriate minisrews and the safe zone for miniscrew placement.
Material and methods
The CBCT images of 60 adults (18 men, 42 women; average age, 26.0 ± 7.8 years) with no craniofacial anomalies or systemic diseases were randomly obtained from the orthodontic patients in the Department of Orthodontics of the Stomatology Hospital at the Fourth Military Medical University, Xi’an, Shaanxi, China. Dental arches with severe crowding, missing teeth, or radiographic signs of periodontal disease were excluded. All scans were taken using a CBCT apparatus (NewTom, Verona, Italy) at 110 kV and 0.07 mA. The CBCT images were formatted into standard DICOM images and reconstructed into continuous slices at 0.3-mm thickness each. Approval was obtained from the institutional review board of the Stomatological Hospital of the Fourth Military Medical University of China (2015033).
Mimics software (version 17.0; Materialise, Leuven, Belgium) was used for the CBCT image analyses. The CBCT images of the maxilla were not distorted or magnified and were displayed simultaneously with their coronal, axial, and sagittal slices so that the maxillary posterior tooth regions could be accurately measured in 3 dimensions.
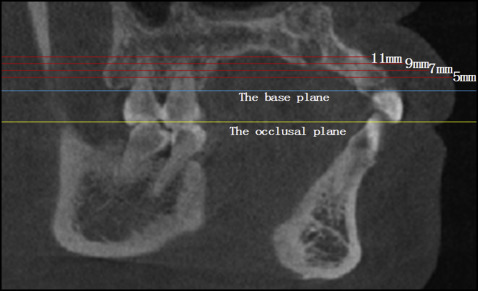
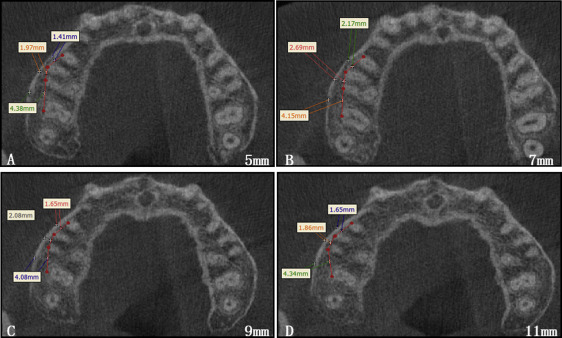
To assess the buccolingual space of miniscrews implanted in the infrazygomatic zone, 3 apical regions were measured: between the maxillary second premolar and first molar (U5-U6), between the mesiodistal roots of the first molar (U6), and between the first and second molars (U6-U7). The buccal alveolar bone thicknesses of these regions were measured at the planes of 5, 7, 9, and 11 mm from the alveolar crest, parallel to the occlusal plane. The occlusal plane through the pitch of incisor and mesiobuccal cusps of both first molars was used as the reference plane for measurement ( Figs 2 and 3 ).
For measuring the buccal alveolar bone height from the alveolar crest edge to the sinus floor, the reference line was located in the middle of U5-U6, U6, and U6-U7 on the axial images. From the coronal slice view through the reference line and parallel to the long axis of the first molar, the buccal bone height from the sinus floor to the alveolar crest edge was measured ( Fig 4 ).
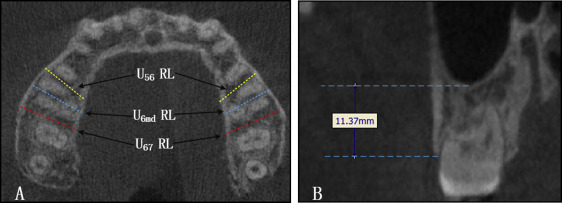
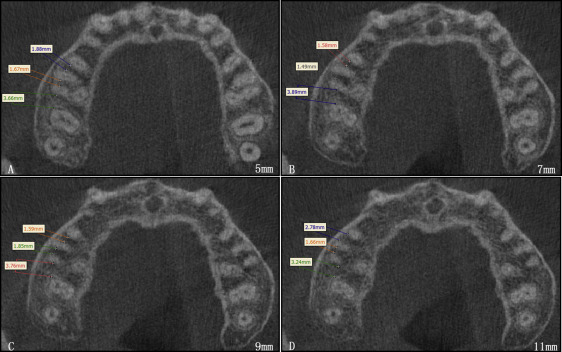
The interdental root distance at the buccal side was measured in the regions of U5-U6, U6, and U6-U7 at the planes of 5, 7, 9, and 11 mm from the alveolar crest edge ( Figs 2 and 5 ).
Measurements and analyses of the data were carried out by 1 researcher (H.L.). Ten volumetric tomographic images of the maxillary region were selected randomly and measured twice at an interval of 2 weeks by the same person. When assessed with the intraclass correlation coefficient, no statistical difference was found between repeated measurements; the results showed that the measurements were reliable ( P >0.05).
Statistical analysis
The data were analyzed using software (version 17.0; SPSS, Chicago, Ill). The Kruskal-Wallis H test was applied to evaluate the differences at each slice in the 3 regions. The statistical significance was determined at α = 0.05.
Results
The means and standard deviations of buccal alveolar bone thickness at the different planes are shown in Table I . There was a significant difference in the buccal alveolar bone thickness among the regions of U5-U6, U6, and U6-U7 at the same plane ( P <0.05). The buccal alveolar bone was thicker in the U6-U7 region than in the U6 and U5-U6 regions. The buccal alveolar bone tended to get thicker from U5-U6 to U6 and U6-U7. There was no significant difference for the buccal alveolar bone thickness at the different planes of each region ( P >0.05). The buccal alveolar bone tended to get thicker from the crest edge to the maxillary sinus floor. The U6-U7 region had the thickest buccal alveolar bone of 4.07 mm at the plane of 11 mm. The U5-U6 region had the thinnest buccal alveolar bone of 1.56 mm at the plane of 5 mm.
| 5 mm | 7 mm | 9 mm | 11 mm | |
|---|---|---|---|---|
| U5b-U6mb | 1.56 | 1.61 | 1.73 | 1.86 |
| SD | 0.24 | 0.30 | 0.26 | 0.36 |
| U6mb-U6db | 2.24 | 2.48 | 2.83 | 3.05 |
| SD | 0.58 | 0.57 | 0.52 | 0.58 |
| U6db-U7mb | 3.04 | 3.41 | 3.69 | 4.07 |
| SD | 0.55 | 0.49 | 0.54 | 0.74 |
There was no significant difference in buccal alveolar bone height for the 3 measured regions of U5-U6, U6, and U6-U7 ( P >0.05). The mean height was more than 10 mm in all 3 regions. The minimum height was 4.21 mm in the U6-U7 region, and the maximum height was 29.32 mm in the U5-U6 region. The buccal alveolar bone height varied greatly because of individual differences. In the 60 subjects, the ratios of the height smaller than 10 mm from the crest edge to the sinus floor were 38%, 52%, and 43% for the regions of U5-U6, U6, and U6-U7, respectively ( Table II ).


