Introduction
The aim of the study was to elucidate whether a newly developed, minimally invasive procedure, piezopuncture, would be a logical modification for accelerating tooth movement in the maxilla and the mandible.
Methods
Ten beagle dogs were divided into 2 groups. Traditional orthodontic tooth movement was performed in the control group. In the experimental group, a piezotome was used to make cortical punctures penetrating the gingiva around the moving tooth. Measurements were made in weeks 1 through 6. Tooth movement and bone apposition rates from the histomorphometric analyses were evaluated by independent t tests.
Results
The cumulative tooth movement distance was greater in the piezopuncture group than in the control group: 3.26-fold in the maxilla and 2.45-fold in the mandible. Piezopuncture significantly accelerated the tooth movements at all observation times, and the acceleration was greatest during the first 2 weeks for the maxilla and the second week for the mandible. Anabolic activity was also increased by piezopuncture: 2.55-fold in the maxilla and 2.35-fold in the mandible.
Conclusions
Based on the different effects of piezopuncture on the maxilla and the mandible, the results of a clinical trial of piezopuncture with optimized protocols might give orthodontists a therapeutic benefit for reducing treatment duration.
Various surgical interventions on the periodontal tissues have been developed to accelerate orthodontic tooth movement. The degree of intentional surgical damage needed to evoke a long-lasting regional acceleratory phenomenon that is less prone to complications has been a topic of special interest. Full-thickness flap elevation with extensive decortications, including various modifications of corticotomies, are undoubtedly effective in increasing cellular activities related to tooth movement. The mechanism of accelerated tooth movement by a regional acceleratory phenomenon depends mainly on transient osteopenia by an accelerated demineralization-remineralization process, providing a more pliable environment, which is distinct from bony block movement in corticotomy-facilitated orthodontics ; therefore, development of a simple procedure just for cortical activation rather than cortical removal is required.
Corticision (patent 0843344, class 10; Kyung Hee University, Seoul, Korea) was introduced as a minimally invasive alternative for cortical activation. A cortical incision made by malleting a reinforced scalpel to separate the interproximal cortices transmucosally was found to induce the regional acceleratory phenomenon effect for faster tooth movement in beagle dog experiments. To mitigate the patients’ fear and discomfort from repeated malleting, Dibart et al suggested “piezocision,” a process that uses an ultrasonic tool to produce the incisions. This procedure combines piezoelectric cortical incisions with selective tunneling, which allows additional tissue grafting.
To overcome the insufficiencies of these earlier procedures, we conceived a novel procedure for cortical activation that we called “piezopuncture.” In this procedure, an ultrasonic tool, a piezotome, is used to create multiple cortical punctures through the overlying gingiva. The concept of ultrasonic osteotomy is based on the so-called reciprocal piezo effect: voltage is applied to a polarized piezo ceramic to deform a piezoelectric crystal in the resultant electrical field; this creates alternating and perpendicular expansion and contraction of the material. Because of its accurate and selective capability of cutting mineralized tissues without damaging adjacent soft tissues and nerves, ultrasonic osteotomes were first used in periapical oral surgery, including implantology and periodontology. These transmucosal manipulations of alveolar bone have minimized morbidity and achieved similar results to more aggressive procedures, including extensive flap elevation for rapid tooth movement.
The aim of our study was to elucidate whether piezopuncture would elicit the regional acceleratory phenomenon and accelerate tooth movement without causing harmful tissue responses. The acceleration rates of tooth movement and bone remodeling were investigated and compared between the maxilla and the mandible.
Material and methods
Ten male beagles (age, 18-24 months; weight, 9-12 kg) were housed in separate cages supplied with a self-washing system, air conditioning, and lighting according to the guidelines of the Institutional Animal Care and Use Committee, Kyung-Hee University Medical Center. The dogs were randomly divided into 2 groups: control (n = 4) and piezopuncture (n = 6). These groups were further divided into 3 subgroups based on the duration of force application: group I, 14 days (control, n = 1; piezopuncture, n = 2); group II, 28 days (control, n = 1; piezopuncture, n = 2); and group III, 42 days (control, n = 2; piezopuncture, n = 2). Each animal provided 4 specimens (1 each from the right and left sides of both jaws), and the maxillary and mandibular specimens (n = 20 for each jaw) were randomly divided into 2 groups. Animals in the control group received orthodontic force alone, and the animals in the piezopuncture group received orthodontic force with piezopuncture. The animals were killed at 2, 4, and 6 weeks after the interventions.
The target teeth in both arches were the second premolars; however, the anchorage teeth in each arch were selected differently because of anatomic limitation. In the maxillary arch, the second premolars were protracted against the canines as the anchorage, whereas the second premolars were retracted against the third premolars in the mandibular arch. Orthodontic buttons (Ormco, Orange, Calif) connected by a lever arm were bonded on the labial surfaces of all experimental teeth with Super-Bond C&B resin (Sun Medical, Shiga, Japan). A nickel-titanium closed-coil spring (Tomy International, Tokyo, Japan) was activated and ligated between the lever arms of the target teeth and the anchorage teeth. For reinforcing anchorages, resin bridges were constructed on the adjacent teeth. The orthodontic force by the appliance was 100 g at the beginning of the experiment. Tooth movement was allowed for 6 weeks. Force magnitude was measured using a force gauge (Haag-Streit, Koeniz, Switzerland) once a week with reactivation of the appliance to maintain a continuous force ( Fig 1 , A ).

For piezopuncture, a piezosurgical instrument with a sharp curved tip (Endo2 insert, ProUltra; Dentsply Maillefer, Ballaigues, Switzerland) was used to perform the cortical punctures penetrating the gingiva. The depth of cortical injury was 3 mm, by holding the tip perpendicular to the gingiva for 5 seconds under saline-solution irrigation. The setting selected for each puncture was in accordance with the manufacturer’s recommendation. Piezopunctures were performed on the mesiobuccal, distobuccal, mesiolingual, and distolingual sides of the second premolars ( Fig 1 , B ). Sixteen punctures were made on 1 target tooth. Gentamicin (7.5 mg/kg) was injected postoperatively for 3 days. Tooth brushing and daily hexamedine (Bukwang, Seoul, South Korea) irrigation were repeated during the postoperative care.
Tooth movement was measured by a digital caliper (Mitutoyo, Kawasaki, Japan) on the stone models once a week. In the maxillary arch, the distance from the mesial cervix of the third premolar to the mesial cervix of the moved second premolar was measured over time. In addition, the distance of canine retraction as an anchorage tooth was measured from the mesial cervix of the third premolar to consider the rate of tooth movement as the relative ratio. In the mandibular arch, the distance from the mesial cervix of the canine to the mesial cervix of the moved second premolar was measured, and the protracted distance of the anchored third premolar was also measured from the same reference. The relative values of the distance of the moved teeth divided by the distances of the anchorage teeth were compared between the groups.
Histologic analysis was performed on the decalcified specimens at 2, 4, and 6 weeks. Tissue blocks including the second premolar with surrounding alveolar bone and the injury site were decalcified with 10% EDTA-2Na (pH 7.4) at 48°C for 30 days. The specimens were resected at 3 to 4 mm below the alveolar crest with thicknesses of 6 μm. The sections were stained with hematoxylin and eosin for descriptive histology.
Quantitative histomorphometric analysis was done on the nondecalcified specimens of the dogs in the 6-week groups. One experimental animal and 1 control animal were randomly selected. They had been intramuscularly injected with 3 fluorochoromes as follows: oxytetracycline hydrochloride (yellow orange, 30 mg/kg; Fluka Chemie AG, Buchs, Switzerland) at 24 hours before intervention and at 6 weeks after intervention; calcein (green, 10 mg/kg; Fluka Chemie AG) at 2 weeks after intervention; and alizarin red (red, 30 mg/kg; Fluka Chemie AG) at 4 weeks after intervention. Specimens were taken from 8 sampling sites in each jaw. These specimens were longitudinally sectioned parallel to the direction of orthodontic traction and examined under an ultraviolet fluorescence microscope (BH-2; Olympus, Tokyo, Japan) with an ultraviolet filter (λ = 515 nm). Microphotographs of all specimens were recorded using a digital CCD camera (PS30C ImageBase; Kappa Optronics, Gleichen, Germany). The outlines of labeled bones were traced from the photographs, and the distances between the labeled lines were measured with image analysis software (ImageBase Metreo 2.5; Kappa Optronics).
Statistical analysis
Descriptive statistics were represented as means and standard deviations for all parameters in each group. The normality of the data was assessed with the Kolmogorov-Smirnov test. Statistical homogeneity was checked using the Levene test. Independent t tests were used to evaluate the intergroup differences of the mean tooth movement distances on the models and the mean accumulated new bone deposition measured by histomorphometric analysis. Values of P <0.05 were considered statistically significant.
Results
The mean cumulative distances of tooth movement for 6 weeks as well as the ratios of target tooth movement to anchorage loss were significantly increased in the piezopuncture groups as opposed to the control groups in both the maxilla and the mandible ( Table I ). The distance of the maxillary second premolar movement in the piezopuncture group (2.31 ± 0.82 mm) was 3.26-fold greater than that in the control group (0.72 ± 0.06 mm). The distance of the mandibular second premolar movement in the piezopuncture group (1.33 ± 0.28 mm) was 2.45-fold greater than that in the control group (0.51 ± 0.19 mm). There was no significant difference in the amount of anchorage tooth movement between the piezopuncture group (maxilla, 1.11 ± 0.12 mm; mandible, 0.46 ± 0.13 mm) and the control group (maxilla, 1.09 ± 0.07 mm; mandible, 0.40 ± 0.13 mm). The relative ratios of maxillary tooth movement were 2.15 ± 0.98 in the piezopuncture group and 0.66 ± 0.02 in the control group. The ratios of mandibular tooth movement were 3.30 ± 1.03 in the piezopuncture group and 1.35 ± 0.75 in the control group.
| Jaw | Group | Beagle site | Second premolar movement, A (mm) | Anchor tooth movement, B (mm) | Ratio (A/B) |
|---|---|---|---|---|---|
| Maxilla | Control (A) | A1-RT | 0.79 | 0.98 | 0.81 |
| A1-LT | 0.74 | 1.12 | 0.66 | ||
| A2-RT | 0.65 | 1.15 | 0.57 | ||
| A2-LT | 0.71 | 1.10 | 0.65 | ||
| Mean | 0.72 ± 0.06 | 1.09 ± 0.07 | 0.67 ± 0.10 | ||
| Piezopuncture (B) | B1-RT | 2.62 | 1.01 | 2.59 | |
| B1-LT | 3.32 | 1.07 | 3.10 | ||
| B2-RT | 1.57 | 1.28 | 1.23 | ||
| B2-LT | 1.71 | 1.07 | 1.60 | ||
| Mean | 2.31 ± 0.82 | 1.11 ± 0.12 | 2.13 ± 0.86 | ||
| P value | 0.00054 ‡ | 0.27102 | 0.00215 † | ||
| Mandible | Control (A) | A1-RT | 0.56 | 0.38 | 1.47 |
| A1-LT | 0.76 | 0.59 | 1.29 | ||
| A2-RT | 0.35 | 0.28 | 1.25 | ||
| A2-LT | 0.38 | 0.35 | 1.09 | ||
| Mean | 0.51 ± 0.19 | 0.40 ± 0.13 | 1.28 ± 0.16 | ||
| Piezopuncture (B) | B1-RT | 1.71 | 0.31 | 5.52 | |
| B1-LT | 1.35 | 0.56 | 2.41 | ||
| B2-RT | 1.12 | 0.58 | 1.93 | ||
| B2-LT | 1.13 | 0.39 | 2.90 | ||
| Mean | 1.33 ± 0.28 | 0.46 ± 0.13 | 3.19 ± 1.60 | ||
| P value | 0.00041 ‡ | 0.55436 | 0.04373 ∗ |
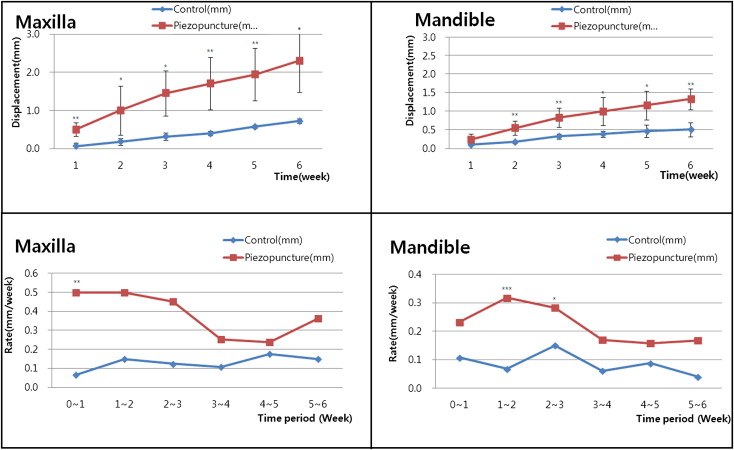
With respect to movement rate, the first 2 weeks in the maxilla and the second week in the mandible had the greatest movement ( Fig 2 ). The weekly velocity of tooth movement in the piezopuncture group was larger than that in the control group at all observation times. The increasing pattern of the accumulated distances of tooth movement in the piezopuncture group showed no remarkable stagnation indicating the lag phase.
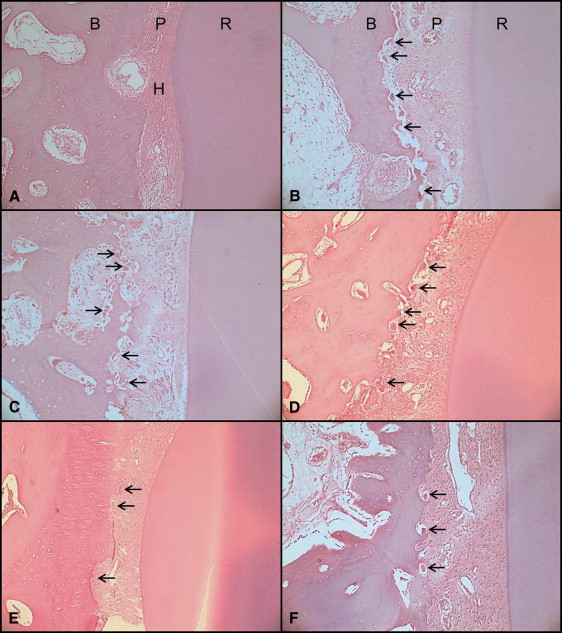
Descriptive histologic findings on the compression sides of moving teeth are shown in Figure 3 . At week 2, the periodontal ligament was compressed and locally degenerated into hyalinization in the control group, where no apparent resorptive findings on the alveolar surfaces were observed ( Fig 3 , A ). In the piezopuncture group, osteoclasts with the resorption lacunae along the bone surfaces were seen near hyalinized areas of the periodontal ligament ( Fig 3 , B ). At week 4, indirect resorption followed by the removal of the hyalinized periodontal ligament was found in the control group ( Fig 3 , C ), whereas direct resorption by active bone-resorbing cells continued in the piezopuncture group ( Fig 3 , D ). At week 6, the number and the activity of bone-resorbing cells were decreased, showing sparse resorption areas on the bone surface with focal hyalinization in the control group ( Fig 3 , E ), whereas the findings of direct bony resorption with the cellular periodontal ligament were as before in the piezopuncture group ( Fig 3 , F ). There were no recognizable differences of the time-dependent histologic responses between the maxilla and the mandible.