Introduction
The purposes of this study were to investigate the relationship between occlusal vertical dimension (VD) changes and postsurgical skeletal changes in the surgery-first approach and to derive regression models for the final mandibular setback at B-point.
Methods
This retrospective study included 40 patients (16 men, 24 women; ages, 22.6 ± 4.0 years) who had undergone a bimaxillary surgery-first approach. Using cephalograms generated from cone-beam computed tomography representing the presurgical, postsurgical, and posttreatment stages, skeletal landmarks in the maxilla and mandible were investigated to derive multivariate linear regression-based prediction models. Additionally, a patient classification based on the VD was established and verified to generate regression models for the classified groups.
Results
For the nonincreased VD group, the surgical setback of B-point was its predictor for the final mandibular setback ( R 2 at 92%). Meanwhile, the final mandibular setback of the increased VD group was predicted according to the surgical upward movement of pogonion, the postsurgical horizontal position of A-point, and the postsurgical vertical position of the coronoid process ( R 2 at 94%).
Conclusions
The results of this study support the clinical observation that the more increased the vertical occlusal dimension after surgery, the less predictable the position of B-point at the posttreatment stage.
Highlights
- •
We used CBCT-generated cephalograms with the superimposition.
- •
We investigated the relationship between vertical dimension changes and postsurgical changes in the surgery-first approach.
- •
The more increased the vertical dimension after surgery, the less predictable the B-point position.
The surgery-first approach (SFA) is characterized by minimal presurgical orthodontic treatment and orthognathic surgery followed by postsurgical orthodontic treatment. The application of SFA has recently been increasing with the publication of reports emphasizing its advantages, which include increased patient cooperation, effective compensation, and a shortened treatment period. However, because presurgical orthodontic treatments such as dental decompensation and arch coordination are rarely performed in the SFA, postsurgical occlusal instability clinically leads to more severe forward postoperative mandibular movement than in conventional surgical orthodontic treatment for patients with a skeletal Class III deformity. Accordingly, the surgical treatment objective for the SFA, often designated as mandibular setback from the horizontal B-point position at the presurgical stage (T0) to the position at the removal of the orthodontic appliance at the posttreatment stage (T2), is not equivalent to the extent of the surgical mandibular setback at T0 to the position immediately after surgery (T1), because of the extent of postoperative mandibular movement from T1 to T2 during active orthodontic treatment. This complicates accurate prediction and simulation of postoperative orthodontic treatment. Therefore, clinical experience is needed for accurate prediction of postoperative orthodontic treatment and assessment of skeletal discrepancy.
As for conventional orthognathic surgery, the gonial angle and the mandibular occlusal plane angle have been suggested to correlate with mandibular relapse. Ko et al, contrastingly, reported overbite to be a predictor of the extent of vertical mandibular relapse in the SFA. However, in their study, overbite was found to explain only 25.9% of the variation of vertical mandibular relapse, leaving the remaining 74.1% unexplained. Moreover, to support the clinical observation that an increased occlusal vertical dimension (VD) at T1 is related to a strong likelihood of more severe postsurgical mandibular forward movement in the SFA, the factors related to postoperative skeletal changes should be investigated. Among them, the relationship of occlusal VD changes to postoperative skeletal changes is especially relevant.
Therefore, the purposes of this study were to investigate the relationship between VD changes and postsurgical skeletal changes in the SFA to orthodontic treatment and to estimate the extent of final mandibular setback (ΔT2-T0). The specific aims of the study were (1) to derive a prediction model of the final mandibular setback extent at B-point (ΔT2-T0) as the sum of the observed surgical setback (ΔT1-T0) and the postoperative mandibular forward movement (ΔT2-T1), and (2) to assess the correlation between VD changes and mandibular movements during postoperative orthodontic treatment to support the clinical significance of postsurgical VD change.
Material and methods
This study was a retrospective study of 40 patients with skeletal Class III deformities (16 men, 24 women; mean age, 22.6 ± 4.0 years) who had undergone bimaxillary surgery with the SFA in the Departments of Oral & Maxillofacial Surgery and Orthodontics at Pusan National University Hospital in South Korea. The exclusion criteria were patients with extractions, severe facial asymmetry, cleft lip and palate, and temporomandibular joint disorders ( Table I ). LeFort I osteotomy and modified Hunsuck sagittal split ramus osteotomy with rigid internal fixation were performed on all patients by 2 surgeons (D.-S.H. and Y.-I.K.), followed by active orthodontic treatment an average of 1 month later. This study was reviewed and approved by the institutional review board of Pusan National University Hospital (E-2011069).
| Overall group, mean (SD) | Nonincreased VD group, mean (SD) | Increased VD group, mean (SD) | |
|---|---|---|---|
| Sample size (n) | 40 | 29 | 11 |
| Sex | 24 women, 16 men | 15 women, 14 men | 9 women, 2 men |
| Mean age (y) | 22.6 (4.0) | 21.9 (3.5) | 24.4 (5.0) |
| Maxillary surgical setback (mm) ∗ | 0.5 (2.3) | 0.4 (2.5) | 0.8 (1.9) |
| Mandibular surgical setback (mm) † | −8.4 (5.7) | −8.7 (6.1) | −7.3 (4.3) |
| Final mandibular setback (mm) ‡ | −7.6 (4.7) | −7.8 (5.1) | −7.1 (3.6) |
∗ Horizontal movement of A-point from T0 to T1 (A 10 ).
† horizontal movement of B-point from T0 to T1 (B 10 ).
‡ final mandibular setback measured as horizontal movement of B-point from T0 to T2 (B 20 ).
Preliminarily, predictor-variable data were compiled as 2-dimensional coordinates of each skeletal landmark, extracted from cephalograms generated by cone-beam computed tomography (CBCT) with ray-cast and maximum intensity projection using CBCT superimposition ( Fig 1 ). CBCT images (DCT Pro; Vatech, Seoul, Korea) were obtained at T0, T1, and T2 with the scanner set at a 20 × 19-cm field of view, 90 kVp, 4.0-mA tube current, and scan time of 24 seconds. To create CBCT-generated half-cephalograms, the CBCT data were reformatted to 3-dimensional images with imaging software (Ondemand 3D; Cybermed, Seoul, Korea), superimposed on the anterior cranial base to obtain ray-cast and maximum intensity projection from the right side of the subjects, and digitized by software (V-ceph version 6.0; Osstem Implant, Seoul, Korea). All measurements were repeated 2 weeks later by the same investigator (J.L.), and the measured data were validated according to the systematic intraexaminer error, with the mean of the 2 measurements used to calculate the corresponding distances of each landmark from the Frankfort horizontal (FH) and sella-perpendicular (S-perp) planes, respectively. The intraclass correlation coefficient for the systematic intraexaminer error was 0.994 (0.990-0.996), and the intraobserver reliability was high for all measurements.
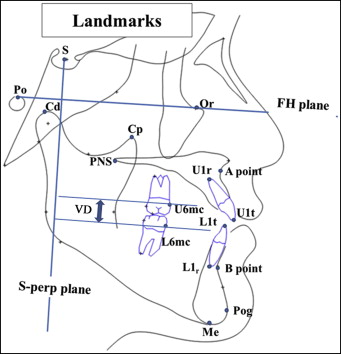
Then, using the coordinates obtained at T0, T1, and T2, both the horizontal and the vertical distances of each landmark from the reference planes were calculated, along with the corresponding increment or decrement in such distances over the periods of T0 to T1 (ΔT1-T0) and T1 to T2 (ΔT2-T1); the corresponding predictor variables were designated as surgical movement (ΔT1-T0) and postsurgical movement (ΔT2-T1) of each landmark. As for the horizontal position of B-point, the change in its distance from the S-perp plane from T0 to T2 (ΔT2-T0) was calculated ( Fig 1 , Table II ).
| Terms | Definitions |
|---|---|
| Landmarks | |
| B-point (B) | Innermost curvature from chin to alveolar bone junction |
| Menton (Me) | Lowest point on symphysis of mandible |
| Pogonion (Pog) | Most anterior point on contour of chin |
| A-point (A) | Innermost curvature from maxillary anterior nasal spine to crest of maxillary alveolar process |
| Coronoid process (Cp) | Tip of coronoid process |
| Planes | |
| Frankfort horizontal (FH) plane | Plane formed by right Pog and both sides of orbitale |
| Midsagittal reference (MSR) plane | Perpendicular to FH plane and passing through nasion and basion |
| S-perpendicular plane (S-perp) | Perpendicular to FH and MSR planes and passing through sella |
| Distances | |
| B-point to S-perp (B s ) | Distance from B-point to S-perpendicular plane |
| Menton to S-perp (Me s ) | Distance from menton to S-perpendicular plane |
| Pogonion to FH plane (Pog f ) | Distance from pogonion to FH plane |
| A-point to S-perp (A s ) | Distance from A-point to S-perpendicular plane |
| Coronoid process to FH plane (Cp f ) | Distance from tip of coronoid process to FH plane |
| Occlusal vertical dimension (VD) | Distance from mesial contact of mandibular first molar to that of maxillary first molar as projected onto S-perpendicular plane |
| Indicators | |
| Final setback of B-point ( Bs20Bs20 B 20 s ) |
B s changes from T0 to T2, final mandibular movement over presurgical (T0) to posttreatment period (T2) |
| Surgical setback of B-point ( Bs10Bs10 B 10 s ) |
B s changes from T0 to T1, surgical movement over presurgical (T0) to postsurgical period (T1) |
| Surgical setback of menton ( Mes10Mes10 Me 10 s ) |
Me s changes from T0 to T1, surgical movement over presurgical (T0) to postsurgical period (T1) |
| Surgical upward movement of pogonion ( Pogf10Pogf10 Pog 10 f ) |
Pog f changes from T0 to T1, surgical movement over presurgical (T0) to postsurgical period (T1) |
| Postsurgical horizontal position of A-point ( As1As1 A 1 s ) |
Distance from A-point to S-perpendicular plane measured at T1 |
| Postsurgical vertical position of coronoid process ( Cpf1Cpf1 Cp 1 f ) |
Distance from tip of coronoid process to FH plane measured at T1 |
| Patient classification criteria | |
| Vertical occlusal dimension (VD) | Distance from mesial contact of mandibular first molar to that of maxillary first molar |
| Nonincreased VD | VD measured at T1 not increased from VD at T0 |
| Increased VD | VD measured at T1 increased from VD at T0 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


