Introduction
Even though the use of titanium miniscrews to provide orthodontic anchorage has become increasingly popular, there is no universally accepted screw-placement protocol. Variables include the presence or absence of a pilot hole, placement through attached or unattached soft tissue, and angle of placement. The purpose of this in-vitro study was to test the hypothesis that screw angulation affects screw-anchorage resistance.
Methods
Three-dimensional finite element models were created to represent screw-placement orientations of 30°, 60°, and 90°, while the screw was displaced to 0.6 mm at a distance of 2.0 mm from the bone surface. In a parallel cadaver study, 96 titanium alloy screws were placed into 24 hemi-sected maxillary and 24 hemi-sected mandibular specimens between the first and second premolars. The specimens were randomly and evenly divided into 3 groups according to screw angulation (relative to the bone surface): 90° vs 30° screw pairs, 90° vs 60° screw pairs, and 30° vs 60° screw pairs. All screws were subjected to increasing forces parallel to the occlusal plane, pulling mesially until the miniscrews were displaced by 0.6 mm. A paired-samples t test was used to assess the significance of differences between 2 samples consisting of matched pairs of subjects, with matched pairs of subjects including 2 measurements taken on the same subject. One-way analysis of variance (ANOVA) with the post-hoc Tukey studentized range test was conducted to determine whether there were significant differences, and the order of those differences, in anchorage resistance values among the 3 screw angulations at maxillary and mandibular sites.
Results
The finite element analysis showed that 90° screw placement provided greater anchorage resistance than 60° and 30° placements. In the cadaver study, although the maximum anchorage resistance provided by screws placed at 90° to the cadaver bone surface exceeded, on average, the anchorage resistance of the screws placed at 60°, which likewise exceeded the anchorage resistance of screws placed at 30°, these differences were not statistically significant.
Conclusions
Placing orthodontic miniscrews at angles less than 90° to the alveolar process bone surface does not offer force anchorage resistance advantages.
The use of titanium miniscrews to provide orthodontic anchorage has become increasingly popular. In a 2008 survey of over 500 orthodontists, it was found that 80% had at least 1 active case involving miniscrews. Compared with traditional endosseous implants, which require time for osseointegration and a second surgical procedure (trephination) for removal, miniscrews can be loaded immediately, are smaller, are easier to place, can be placed in more varied locations, are more cost effective, and result in less postoperative pain. However, in spite of their wide acceptance and ease of use, there is no universally accepted screw-placement protocol, and placement variables can include the presence or absence of a pilot hole, placement through attached or unattached soft tissue, and angle of placement.
The primary stability of miniscrews is believed to result from mechanical interlock and be determined by factors such as cortical quality and quantity, soft-tissue health, operator technique, and screw diameter. Several authors have suggested placing orthodontic mini-implants at an angle to the surface of the cortical bone not only to help the screw avoid tooth roots but also to provide increased screw-to-cortical bone contact. Wilmes et al, measuring placement torque as a sign of primary stability in vitro, measured placement torque at 7 angles (30°, 40°, 50°, 60°, 70°, 80°, and 90°) in ilium bone segments of pigs. They concluded that, to achieve the best primary stability, a placement angle of 60° to 70° is advisable. In 1 clinical study, it was suggested that placement of miniscrews at an angle to the bone surface gave more cortical bone contact and allowed for longer screws to be placed with no significant difference in success rates based on angulation. This was supported by another study recommending placement of miniscrews in the mucogingiva at an angulation of 30° to 45°. Deguchi et al, using computed tomographic scanning to measure cortical thickness, concluded that placing the implant at approximately 30° to the long axis of the tooth would increase cortical bone contact by as much as 1.5 times compared with placement at 90°.
These studies suggest that placement of a miniscrew at an angle to the bone surface increases cortical bone contact and placement torque, which might have a positive effect on miniscrew stability. However, angulated (as opposed to perpendicular) miniscrew placement can create a different problem. Regardless of placement angle, a miniscrew must be placed with the head a fixed perpendicular distance from the bone surface so that the miniscrew head is located above the soft tissues to allow force engagement. Therefore, having a miniscrew exit the bone at an angle other than 90° potentially creates a longer lever arm for the applied force. The effect of a longer lever arm could negatively balance, or even outweigh, any positive effect of increased bone contact with an angulated screw. Thus, a question still remains: what is the effect of miniscrew angulation on anchorage resistance? The literature does not provide the answer to this question. The purpose of this in-vitro study was to test the hypothesis that orthodontic miniscrew angular placement impacts screw-anchorage resistance.
Material and methods
Three-dimensional finite element models were created to represent screw placement orientations of 30°, 60°, and 90°. Each mesh consisted solely of hexahedral elements modeled by using IA-FEMesh, and, in each model, the screw was represented by a cylinder with a diameter of 1.5 mm. The screws were modeled as a titanium alloy with an elastic modulus of 110 gigapascals (GPa) and Poisson’s ratio of 0.34. A section of bone measuring 9.5 mm long, 8.15 mm high, and 6 mm thick was considered. The cortical layer measured 1.79 mm thick and was assigned an elastic modulus of 13.7 GPa, and the elastic modulus of the trabecular bone was 200 megapascals (MPa). The bone was assumed to be homogenous and isotropic with a Poisson’s ratio of 0.3. The contact between the bone and the screw was defined as a frictional interface with a coefficient of friction of 0.37. The superior, inferior, and lingual nodes of the bony elements were fixed completely, and the screw was displaced to 0.6 mm at a distance of 2.0 mm from the bone surface.
The maxillae and mandibles of human cadavers were obtained from the Department of Anatomy and Cell Biology Deeded Body Program at the University of Iowa. Vital statistics of the cadavers were not available. Fully edentulous or partially dentate specimens with severely atrophic alveolar ridges were excluded. All specimens were hemi-sected, soft tissues were carefully removed, and the specimens were stored in 10% buffered formalin solution.
Twenty-four hemi-maxillae from different cadavers and 24 hemi-mandibles from different cadavers were used. The site for placement of screws was in the area between the first and second premolars. Periapical radiographs of each specimen were made before and after placement of the miniscrews to verify that the screws were not encroaching on the neighboring roots, sinuses, or mental foramina.
A total of 96 commercially available screws were placed in the 48 hemi-sected maxilla and mandible specimens. All screws used were 1.5 × 11 mm long (#25-675-11, KLS Martin, Jacksonville, Fla) and were manufactured from titanium alloy (Ti-6Al-4V). The screws were placed to a depth of 6 mm. Coronally positioned screws were placed 4 mm apical to the maximal height of the interproximal crestal bone. The apically positioned screw was placed 5.5 mm apical to the coronally positioned screw ( Fig 1 ). All screws were placed by 1 operator (N.W.) with a hand driver (blade, #25-483-97, and handle, #25-402-99, KLS Martin) after a pilot hole was drilled with the manufacturer’s recommended nontapered, 1.1-mm diameter twist drill for 1.5-mm screws (#25-452-15, KLS Martin).
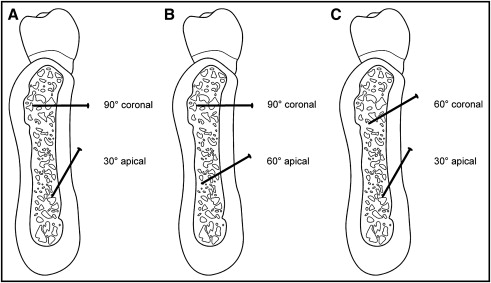
The cadaver specimens were divided into 4 groups (8 hemi-maxillae and 8 hemi-mandibles per group) according to screw placement angulation relative to the bone surface ( Fig 2 ): 90° vs 30° screw pairs, 90° vs 60° screw pairs, and 30° vs 60° screw pairs. In the 3 groups, each angle was used apically in half of the specimens and coronally in half of the specimens. As an example, in the first group, 4 hemi-maxillae had 90° screws placed in the apical position with 30° screws in the coronal positions, and 4 hemi-maxillae had 30° screws in apical positions with 90° screws in coronal positions. After verification of satisfactory screw placement, the most distal portion of each bony specimen was embedded in buff laboratory stone to a depth of 1.0 in and allowed to harden for 24 hours.
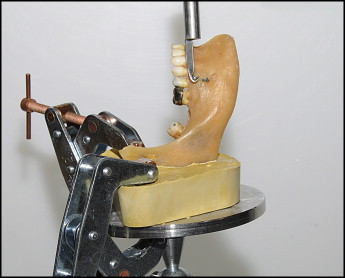
Each miniscrew was subjected to tangential force application oriented parallel to the occlusal plane ( Fig 3 ) to mimic orthodontic tangential force to retract the anterior teeth. An Instron diametral materials testing machine (model 1445, Zwick, Ulm, Germany), incorporating a force transducer attached to a crosshead and linked to a computer for recording data, was used to apply force. A customized X-Y-Z table with a mounting device was fabricated to rigidly fixate each stone block and cadaver specimen during testing. This table allowed for movement in 3 planes of space to ensure that the force was parallel to the occlusal plane. A customized grip was designed and machined from stainless steel to fit between the threads of each miniscrew. The grip was attached to the force transducer, oriented in a vertical position, and attached to each miniscrew at a distance of 2 mm from the screw-bone interface. This distance was selected to represent space that would be expected to be occupied by soft tissues in vivo and the screw head fixtures.