Introduction
Cone-beam computed tomography (CBCT) has been used to assess alveolar bone changes after rapid palatal expansion. The purpose of this study was to investigate the accuracy of alveolar bone-height measurements from CBCT images with varied bone thicknesses and imaging resolutions.
Methods
Eleven maxillary specimens from 6-month-old pigs were measured for alveolar bone height (distance between drilled reference holes and alveolar crests) at 6 locations with a digital caliper, followed by CBCT scanning at 0.4-mm and 0.25-mm voxel sizes. Buccal alveolar bone of these locations was then reduced approximately by 0.5 to 1.5 mm, followed by CBCT rescanning with the same voxel sizes. The CBCT images were measured by using 3-dimensional software to determine alveolar bone height and thickness in buccolingual slices by independent, blinded raters. The specimens were subsequently cut into buccolingual sections at reference-hole levels, and direct bone height and thickness were measured from these sections. Intrarater and interrater repeatability and the differences between CBCT and direct measurements were assessed.
Results
Excellent intrarater (intraclass correlations, r = 0.89-0.98) and good interrater (r = 0.64-0.90) repeatability values were found for alveolar bone-height measurements from the CBCT images. Before alveolar bone reduction, the thickness was much greater than the CBCT voxel size (0.4 mm), and bone-height measurements from the CBCT images were 0.5 to 1 mm more than the direct measurements (paired t tests, P <0.017 at most locations). After bone reduction, the thickness at the subcrest 1-mm level was near or below the CBCT voxel size (0.4 mm), and bone-height measurements from the CBCT images were 0.9 to 1.2 mm less than the direct measurements (paired t tests, P <0.017 at most locations). These measurement inaccuracies were substantially improved by decreasing the CBCT voxel size to 0.25 mm.
Conclusions
Alveolar bone-height measurements from conventional clinical 0.4-mm voxel size CBCT images might overestimate alveolar bone-height loss associated with rapid palatal expansion.
Cone-beam computed tomography (CBCT) has become increasingly popular in many specialties of dentistry. With detailed 3-dimensional (3D) information, CBCT imaging offers clinicians and researchers a novel way to visualize and quantify bone-structure morphology and changes associated with diseases and treatments.
Alveolar bone changes after orthodontic rapid palatal expansion treatment were recently measured by using CBCT images. Strikingly, buccal alveolar bone-height reductions were more than 5 mm for the maxillary first premolars and 3 mm for the maxillary first molars, both anchor teeth for the expander. Although these findings certainly indicate concerns for periodontal tissue compromise caused by palatal expansion, the accuracy of using CBCT imaging to take linear measurements of alveolar bone also needs to be examined.
Several recent studies assessed the accuracy of CBCT linear measurements of skull and jaw bones. In comparison with direct physical measurements, those from CBCT images differed by submillimeters to 4 to 5 mm. For alveolar bone, the accuracy of its linear measurements from CBCT images compared with direct physical measurements has been investigated by using formalin-fixed and dry human specimens, and overall submillimetric inaccuracies were found. Compared with skull and jaw bones, the alveolar bone is much thinner, especially when the thickness was further reduced by orthodontic treatment such as palatal expansion. Image unsharpness and artifacts related to CBCT imaging, such as an inherent partial-volume averaging effect, therefore, can have larger effects on the accuracy of alveolar bone-height measurement in these situations.
The purpose of this study was to assess whether linear alveolar bone-height and thickness measurements can accurately reflect actual alveolar bone dimensions. Specifically, we examined whether alveolar bone-height measurements from CBCT images are affected by alveolar bone thickness and CBCT spatial resolutions. We hypothesized that (1) when alveolar bone thickness is decreased to a near-pixel level, alveolar bone can become indistinguishable from adjacent structures because of the partial-volume averaging effect, resulting in underestimation of alveolar bone-height measurements; and (2) a higher CBCT resolution level (0.25 vs 0.4 mm) produces more accurate alveolar bone linear measurements.
Material and methods
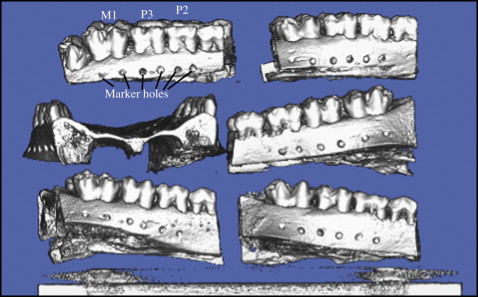
We obtained the frozen heads of 6 domestic pigs ( Sus scrofa ; age, 6 months) from a local vender (Herman Fauter, Columbus, Ohio). The pig was chosen for this study because the anatomy and size of its teeth and alveolar bone are similar to those of humans, and it has been used in palatal expansion studies before. After the heads were thawed, the maxillary bone containing the alveolar bone of the first molar (M1), and the third and second primary molars (P3 and P2) was separated from the skull. All attached soft tissue was removed. By using a dental bur, a straight groove was made at the occlusal surface of M1, P3, and P2 connecting their central fosae, and marker holes were drilled at the buccal alveolar bone at least 4 mm below the alveolar crest and aligned with the distal and mesial cusp tips ( Fig 1 ). Each half maxilla was considered an independent sample. The marker holes piloted in 1 specimen were mistakenly drilled, and this specimen was not used for subsequent analyses, so the total sample size was 11.
By using a digital caliper (precision of 0.01 mm), alveolar bone height was measured from the top edge of each marker hole to its corresponding alveolar bone crest by 1 investigator (Z.S.). After a 30-minute interval, this procedure was repeated, and the 2 sets of measurements were averaged and recorded as direct bone-height measurements before bone reduction.
CBCT images were obtained by using an iCAT scanner (Imaging Science International, Hatfield, Pa). All specimens were first randomly arranged and stacked in 3 layers ( Fig 1 ). The field of view was adjusted to contain all specimens, followed by 2 scans: 1 at 0.4-mm voxel size and the other at 0.25-mm voxel size. The images were reconstructed by software provided by the iCAT system and exported as DICOM format files.
With a dental bur, layers of bone with approximate thicknesses of 1.5 and 0.5 mm were removed from the distal and mesial aspects, respectively, of the buccal cortical plate. The reduction area spanned from the alveolar crest to a point approximately 4 mm subcrestally. The 1.5-mm reduction was aimed at making the remaining bone thickness near or below the CBCT voxel size of 0.4 mm, and the 0.5-mm reduction was aimed at keeping bone thickness much greater than the voxel size after the reduction. These amounts were chosen based on pilot measurements of 1 sample. During the reduction procedure, however, large variations of the original buccal alveolar bone thickness were noticed, and the precise amount of bone-thickness reduction was difficult to achieve.
Direct measurements of postreduction alveolar bone height were made the same way as prereduction measurements.
Postreduction CBCT scans at 0.4-mm and 0.25-mm voxel sizes were conducted in the same fashion as prereduction scans, except that all specimens were rearranged randomly in new positions.
Alveolar bone-height and thickness measurements from the CBCT images were carried out by using Dolphin 3D software (Dophin Imaging and Management Solutions, Chatsworth, Calif). Height measurements were made by 2 raters (T.S. and S.K.) independently. Thickness measurements were made by 2 raters (T.S. and B.C.T.) independently. The identity of the specimens was blinded to all raters. A total of 48 specimen locations were chosen by using a random table and were remeasured after at least a 2-week interval for intrarater agreement tests.
The detailed procedure of alveolar bone measurement is illustrated in Figure 2 . Briefly, DICOM volumetric data were loaded into the Dolphin 3D software. X-ray images were subsequently built with the default setup of the software. No bone-nonbone tissue segmentation was performed. The target specimen was oriented with the occlusal plane parallel with the horizontal plane; buccolingual sections perpendicular to the marker groove at the occlusal surface were obtained; and the 3 images showing the best clarity of each marker hole were used for alveolar bone-height and thickness measurements.
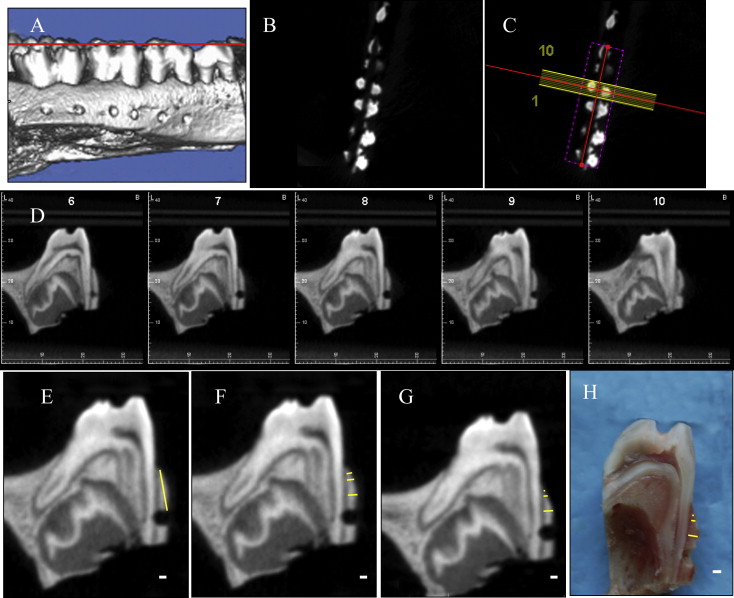
Sections bisecting the marker holes ( Fig 2 , H ) were obtained by using a low-speed diamond-blade saw (Buehler, Lake Bluff, Ill). Alveolar bone thickness at the same locations as the postreduction CBCT images were directly measured by using a digital caliper. Unlike bone-height measurements, made directly with a caliper on both prereduction and postreduction specimens, direct bone thickness could only be measured when the sections were obtained. Prereduction thickness measurements, therefore, were obtained only from the CBCT images.
Statistical analysis
Intrarater and interrater agreement values of CBCT measurements were examined by intraclass correlations (ICC). Intrarater analysis was based on 48 randomly chosen locations, which were measured twice. Interrater analysis was based on all measurements. Bone-height measurements (CBCT 0.4 mm, CBCT 0.25 mm, and direct) before and after bone reduction, and bone-thickness measurements after bone reduction, were compared between 2 conditions by paired t tests. Because of the use of 3 paired analyses, Bonferroni adjustments were performed, and the significance level (α) was determined as 0.017 (0.05/3). Bone thickness before bone reduction was measured only from the 0.4-mm and 0.25-mm voxel size images, and their differences were analyzed by paired t tests with a regular significance level (α = 0.05). All statistical analyses were performed by using PASW Statistics 18 software (SPSS, Chicago, Ill).
Results
Intrarater and interrater agreement values of alveolar bone measurements from the CBCT measurements are shown in Table I . For the height measurements, intrarater agreement was over 0.9, and interrater agreement was over 0.6. The agreement coefficient was not affected by the CBCT resolution levels. Bone-thickness measurements were evaluated only for interrater agreement, which tended to be better than height measurements.
| Intraclass correlations | Prereduction 0.4 mm | Prereduction 0.25 mm |
Postreduction 0.4 mm |
Postreduction 0.25 mm |
Combined |
|---|---|---|---|---|---|
| Intrarater (T.S.) ∗ | 0.96 | 0.97 | 0.97 | 0.89 | 0.94 ∗ |
| Intrarater (S.K.) ∗ | 0.97 | 0.98 | 0.72 | 0.77 | 0.93 ∗ |
| Interrater (height) † | 0.90 | 0.73 | 0.68 | 0.64 | 0.76 |
| Interrater (thickness) † | 0.83 | 0.92 | 0.96 | 0.75 | 0.84 |
∗ Combined intrarater agreement was based on 48 randomly chosen locations for remeasurements
† Combined interrater agreement was based on all height or thickness measurements.
Prereduction bone-height measurements are summarized in Table II . Compared with direct measurements, measurements from the 0.4-mm resolution CBCT images were greater (overestimation) with significance achieved at 4 locations ( P <0.017). The P value for the M1-distal location was also slightly above the significance level. Measurements of the 0.25-mm resolution also tended to be overestimated relative to the direct measurements, but no location reached statistical significance ( P >0.017). Compared with measurements from the 0.4-mm resolution images, the measurements from the 0.25-mm resolution images were significantly less overestimated at all locations ( P <0.017). An example of these differences is shown in Figure 3 , A .
| CBCT 0.4 mm | CBCT 0.25 mm | Direct measurements | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Specimen | M1-D | M1-M | P3-D | P3-M | P2-D | P2-M | M1-D | M1-M | P3-D | P3-M | P2-D | P2-M | M1-D | M1-M | P3-D | P3-M | P2-D | P2-M |
| 1-left | 6.5 † | 6.4 | 7.3 | 7.2 | 8.2 | 8.7 | 6.0 | 5.9 | 6.8 | 6.9 | 7.6 | 8.3 | 5.8 | 5.7 | 6.8 | 6.5 | 7.3 | 8.2 |
| 1-right | 8.6 | 8.6 | 8.9 | 8.4 | 8.8 | 8.5 | 8.1 | 8.2 | 8.2 | 7.9 | 8.0 | 7.8 | 8.1 | 7.8 | 8.0 | 7.8 | 8.0 | 7.9 |
| 2-left | 7.2 | 7.9 | 8.4 | 7.1 | 9.1 | 10.5 | 6.9 | 7.4 | 7.7 | 6.9 | 8.5 | 9.8 | 6.5 | 6.6 | 6.5 | 6.2 | 6.8 | 8.7 |
| 2-right | 6.3 | 6.3 | 7.8 | 6.2 | 7.9 | 7.7 | 5.9 | 5.9 | 7.2 | 6.0 | 7.5 | 7.4 | 6.2 | 6.1 | 7.1 | 6.0 | 6.9 | 7.3 |
| 3-left | 5.5 | 7.2 | 7.6 | 7.1 | 8.0 | 8.0 | 5.0 | 6.6 | 7.5 | 6.9 | 7.7 | 7.3 | 5.4 | 6.3 | 7.3 | 4.7 | 7.2 | 7.0 |
| 3-right | 6.2 | 6.5 | 7.8 | 7.1 | 7.6 | 7.0 | 6.0 | 6.3 | 7.6 | 6.5 | 6.9 | 6.7 | 5.1 | 6.4 | 7.5 | 6.6 | 7.7 | 7.6 |
| 4-left | 8.0 | 8.0 | 8.4 | 7.0 | 6.8 | 9.4 | 7.7 | 7.4 | 7.5 | 6.3 | 6.7 | 8.7 | 7.0 | 7.5 | 7.3 | 6.2 | 5.5 | 6.3 |
| 4-right | 7.0 | 6.7 | 7.0 | 5.6 | 6.4 | 6.2 | 6.6 | 6.1 | 6.7 | 5.4 | 5.9 | 5.9 | 5.9 | 5.7 | 6.8 | 5.3 | 4.8 | 6.1 |
| 5-right | 4.9 | 6.2 | 6.6 | 5.4 | 6.5 | 5.4 | 5.1 | 5.6 | 6.4 | 5.2 | 6.4 | 5.4 | 5.5 | 4.8 | 6.2 | 5.4 | 7.2 | 6.8 |
| 6-left | 5.9 | 5.7 | 7.6 | 6.5 | 8.6 | 8.1 | 5.8 | 5.7 | 7.6 | 6.1 | 8.2 | 7.8 | 5.4 | 5.9 | 7.1 | 6.4 | 6.9 | 7.6 |
| 6-right | 7.6 | 8.0 | 9.0 | 7.1 | 8.4 | 7.7 | 7.4 | 8.1 | 8.9 | 7.0 | 8.3 | 7.5 | 7.7 | 8.5 | 8.0 | 7.0 | 7.6 | 6.7 |
| Mean of overestimation ‡ | 0.4 | 0.6 | 0.7 | 0.6 | 0.9 | 0.6 | 0.2 | 0.2 | 0.3 | 0.3 | 0.5 | 0.2 | ||||||
| SD of overestimation ‡ | 0.5 | 0.6 | 0.5 | 0.7 | 0.8 | 1.1 | 0.5 | 0.4 | 0.4 | 0.7 | 0.8 | 1.0 | ||||||
| Paired t tests § : P | ||||||||||||||||||
| 0.4 vs direct | 0.02 | ∗ | ∗ | ∗ | ∗ | 0.09 | ||||||||||||
| 0.25 vs direct | 0.28 | 0.19 | 0.03 | 0.24 | 0.06 | 0.45 | ||||||||||||
| 0.4 vs 0.25 | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ||||||||||||
† All CBCT measurements were the averages of 2 raters
‡ Overestimation was calculated as the difference between CBCT and direct measurements.
§ Bonferroni adjustment was made based on 3 paired t tests (adjusted probability, α = 0.05/3).
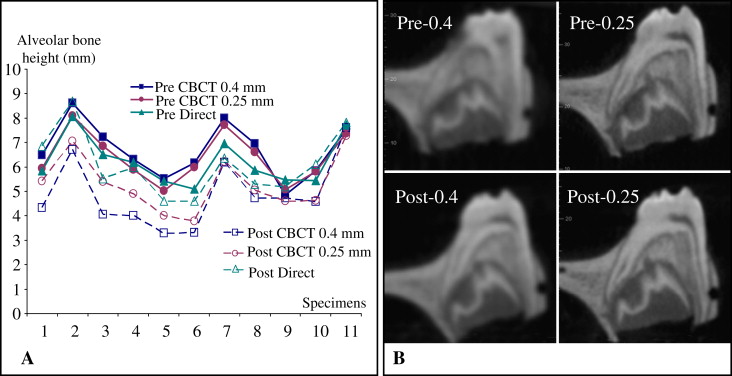
Postreduction bone-height measurements are summarized in Table III . Compared with direct measurements, measurements from the 0.4-mm resolution CBCT images were significantly ( P <0.017) smaller (underestimation) at all locations except for P3-mesial ( P = 0.03). Measurements at the 0.25-mm resolution also tended to be underestimated, with significance ( P <0.017) reached at 2 locations (M1-distal, M1-mesial) and P values less than 0.05 at all other locations. Compared with measurements from the 0.4-resolution images, measurements from the 0.25-resolution images tended to be less underestimated, although only 1 location reached significance. An example (M1-distal) of these differences is shown in Figure 3 , A .
| CBCT 0.4 mm | CBCT 0.25 mm | Direct measurements | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Specimen | M1-D | M1-M | P3-D | P3-M | P2-D | P2-M | M1-D | M1-M | P3-D | P3-M | P2-D | P2-M | M1-D | M1-M | P3-D | P3-M | P2-D | P2-M |
| 1-left | 4.3 † | 5.1 | 5.5 | 6.4 | 6.3 | 8.3 | 5.4 | 5.4 | 6.5 | 6.8 | 6.8 | 8.2 | 6.8 | 6.3 | 7.2 | 7.0 | 8.1 | 6.8 |
| 1-right | 6.7 | 6.9 | 7.3 | 7.7 | 6.8 | 7.2 | 7.1 | 7.1 | 7.6 | 7.8 | 7.7 | 7.8 | 8.7 | 7.8 | 8.5 | 8.2 | 8.7 | 8.7 |
| 2-left | 4.1 | 6.3 | 5.6 | 5.2 | 5.4 | 9.4 | 5.4 | 7.0 | 6.1 | 5.8 | 5.3 | 9.5 | 5.5 | 7.0 | 6.2 | 6.3 | 5.5 | 5.5 |
| 2-right | 4.0 | 5.1 | 5.8 | 4.7 | 6.3 | 6.8 | 4.9 | 5.7 | 6.9 | 5.3 | 6.9 | 7.2 | 6.0 | 6.1 | 7.4 | 5.8 | 8.8 | 6.0 |
| 3-left | 3.3 | 3.3 | 6.8 | 5.9 | 6.3 | 7.2 | 4.0 | 6.2 | 7.6 | 6.4 | 8.0 | 7.6 | 4.6 | 7.1 | 8.0 | 6.6 | 7.7 | 4.6 |
| 3-right | 3.3 | 4.5 | 3.6 | 1.9 | 4.9 | 6.5 | 3.8 | 5.2 | 5.9 | 2.8 | 6.1 | 6.8 | 4.6 | 7.0 | 7.1 | 5.6 | 7.7 | 4.6 |
| 4-left | 6.2 | 7.6 | 6.2 | 5.2 | 5.0 | 4.5 | 6.2 | 7.3 | 6.1 | 5.1 | 4.7 | 4.5 | 6.4 | 7.4 | 7.0 | 4.9 | 4.3 | 6.4 |
| 4-right | 4.7 | 4.1 | 6.1 | 3.9 | 4.2 | 5.7 | 5.1 | 4.9 | 6.4 | 4.2 | 4.3 | 5.7 | 5.3 | 6.3 | 7.8 | 5.7 | 5.3 | 5.3 |
| 5-right | 4.7 | 5.1 | 6.5 | 4.1 | 5.4 | 5.1 | 4.6 | 5.0 | 6.7 | 3.6 | 5.8 | 5.4 | 5.2 | 4.6 | 6.2 | 4.8 | 5.6 | 5.2 |
| 6-left | 4.6 | 5.0 | 6.4 | 6.3 | 6.2 | 8.2 | 4.6 | 5.4 | 7.7 | 6.6 | 6.3 | 8.0 | 6.1 | 5.9 | 7.5 | 6.5 | 6.9 | 6.1 |
| 6-right | 7.6 | 7.6 | 7.7 | 7.3 | 7.6 | 6.9 | 7.3 | 8.1 | 7.8 | 7.1 | 7.7 | 6.9 | 7.8 | 8.0 | 7.6 | 6.9 | 7.4 | 7.8 |
| Mean of underestimation ‡ | −1.2 | −1.2 | −1.2 | −0.9 | −1.1 | −0.7 | −0.8 | −0.6 | −0.5 | −0.6 | −0.6 | −0.5 | ||||||
| SD of underestimation ‡ | 0.8 | 1.2 | 1.0 | 1.2 | 1.1 | 0.7 | 0.5 | 0.7 | 0.6 | 0.9 | 0.8 | 0.7 | ||||||
| Paired t tests § : P | ||||||||||||||||||
| 0.4 vs direct | ∗ | ∗ | ∗ | 0.03 | ∗ | ∗ | ||||||||||||
| 0.25 vs direct | ∗ | ∗ | 0.03 | 0.04 | 0.04 | 0.03 | ||||||||||||
| 0.4 vs 0.25 | 0.02 | 0.04 | ∗ | 0.07 | 0.02 | 0.06 | ||||||||||||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


