Introduction
The aim of the study was to compare the reliability and accuracy of 3 commercially available digital imaging and communications in medicine (DICOM) viewers for measuring upper airway volumes.
Methods
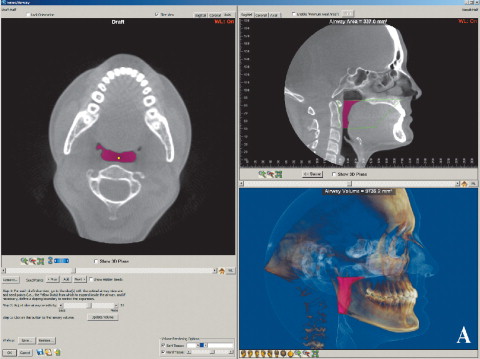
Thirty cone-beam computed tomography scans were randomly selected, and the upper airway volumes were calculated for both oropharynx and nasal passage. Dolphin3D (version 11, Dolphin Imaging & Management Solutions, Chatsworth, Calif), InVivoDental (version 4.0.70, Anatomage, San Jose, Calif), and OnDemand3D (version 1.0.1.8407, CyberMed, Seoul, Korea) were compared with a previously tested manual segmentation program called OrthoSegment (OS) (developed at the Department of Orthodontics at Case Western Reserve University, Cleveland, Ohio). The measurements were repeated after 2 weeks, and the ICC was used for the reliability tests. All commercially available programs were compared with the OS program by using regression analysis. The Pearson correlation was used to evaluate the correlation between the OS and the automatic segmentation programs.
Results
The reliability was high for all programs. The highest correlation found was between the OS and Dolphin3D for the oropharynx, and between the OS and InVivoDental for nasal passage volume. A high correlation was found for all programs, but the results also showed statistically significant differences compared with the OS program. The programs also had inconsistencies among themselves.
Conclusions
The 3 commercially available DICOM viewers are highly reliable in their airway volume calculations and showed high correlation of results but poor accuracy, suggesting systematic errors.
Read the full text online at: www.ajodo.org , pages S50.e1-S50.e9.
Editor’s COMMENT
The limitation of lateral cephalograms regarding the projection of 3-dimensional (3D) structures on a 2-dimensional (2D) film is well known and has been a major issue in studies assessing cross-sectional areas and volumes of the airway. The arrival of 3D cone-beam computed tomography (CBCT) images promised to alleviate this problem, but the new technology needs new tools and validation studies. Measuring in 3D is not as simple as in 2D. To measure the area of the airway in 2D, we need to outline it in only 1 image; in 3D, we need to outline the airway in each of many images (slices), perhaps several hundred. Once the areas are outlined, we measure the number of voxels in each and derive the total volume. Software tools have been developed to make the process faster and easier; their main function is to separate the airway voxels from the rest, a process called segmentation. Automatic segmentation is a notoriously difficult task in computer graphics, especially when the images have noise, as happens in CBCT. Although airway voxels can be darker than soft-tissue or bone voxels, density is not enough to differentiate them, because density values invariably overlap; selecting voxels of a specific density range will invariably ignore some voxels that should be selected and include others that should not be selected. There are various algorithms to avoid such problems, but there is no universally good solution.
These authors assessed 3 commercially available software programs to determine their reliability and accuracy compared with manual segmentation of the airway, which was considered the gold standard. All 3 programs had high reliability, so we would get the same results on repeated measurements. However, all 3 had low accuracy, meaning that the results would not be valid. Differences between manual and automatic segmentation exceeded 30% in some cases. More work needs to be done before automatic airway segmentation can be accepted as a valid procedure.
Demetrios J. Halazonetis
Kifissia, Greece