Introduction
The purpose of this study was to investigate the dimensional changes in each skeletal unit in the mandibles of patients with facial asymmetry and mandibular prognathism.
Methods
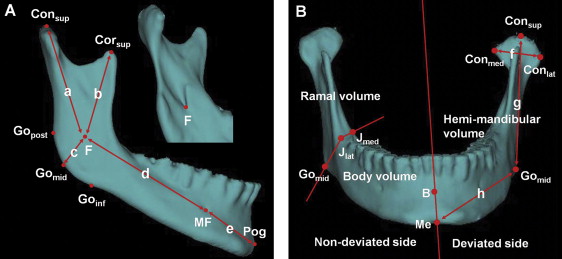
The patients consisted of 50 adults with mandibular prognathism, divided into the symmetry group (n = 20) and the asymmetry group (n = 30) according to the degree of menton deviation. Three-dimensional computed tomography scans were obtained with a spiral computed tomography scanner. Landmarks were designated on the reconstructed 3-dimensional surface models. The lines to represent condylar, coronoid, angular, body, and chin units were used. Ramal and body volumes were measured in the hemi-mandibles.
Results
In the asymmetry group, condylar and body unit lengths were significantly longer, and coronoid unit length was significantly shorter on the nondeviated side than on the deviated side ( P <0.01). Angular and chin unit lengths were not significantly different between the 2 sides ( P >0.05). Ramal volume was significantly greater on the nondeviated side ( P <0.01), but body volume was not significantly different between the 2 sides ( P >0.05).
Conclusions
Both condylar and body units appeared to contribute to mandibular asymmetry, with a more central role of the condylar unit.
Editor’s comment
Clinicians know how common it is to see facial asymmetry in patients with mandibular prognathism. In the United States, facial asymmetry is present in about 34% of the population, and, in subjects with skeletal Class III malocclusion, the rates are even higher—40% in the United States and as high as 42.3% in Korea. Although many studies place the blame for most asymmetries on the mandible, it has been a bit of a guessing game. Melvin Moss saw the mandible as a composite of relatively independent skeletal units including the alveolar, coronoid, angular, and condylar processes along with the body and chin. Which of these components is responsible for creating an asymmetric face? Recent computed tomography examinations of asymmetric patients are helping provide an answer.
Clinical and 2D radiographic examinations were carried out on patients who visited the Yonsei University Dental Hospital between 2005 and 2009. Fifty adults with skeletal Class III malocclusion and mandibular prognathism and no degenerative disease of the temporomandibular joint were studied. The symmetry group consisted of 10 men and 10 women whose menton deviations were less than 2 mm from the midsagittal reference line. The asymmetry group consisted of 15 men and 15 women whose menton deviations were more than 4 mm. The use of 3D CT technology allowed the investigators to (1) observe actual measurements without distortion, regardless of head posture; (2) identify real anatomic surface landmarks for dimensional measurements; and (3) make volumetric measurements.
To summarize the findings, the asymmetry group showed significantly greater differences in condylar unit length, body unit length, coronoid unit length, condylar width, ramal height, body length, hemi-mandibular volume, and ramal volume between the nondeviated and deviated sides compared with the symmetry group, confirming the overall asymmetric morphology of the mandible. However, the difference in condylar unit length was significantly greater than the difference in body unit length. Knowing these differences might help clinicians make better decisions in treating facial asymmetry.