Introduction
Incorrect tongue posture on the mouth floor is considered an important factor in the etiology of unilateral posterior crossbite. The aim of this study was to objectively assess tongue posture in children with unilateral posterior crossbite and those with normal deciduous dentition by using 3-dimensional (3D) ultrasonography.
Methods
First, referential 3D ultrasound images for differently postured tongues were acquired and reconstructed in 10 adults. Second, 27 children with unilateral posterior crossbite (mean age, 5.4 ± 1 years) and 23 children with normal deciduous dentition (mean age, 6.2 ± 0.4 years) were examined by using the 3D ultrasound technique. The referential 3D ultrasound reconstructions were used for the assessment of tongue posture in each child.
Results
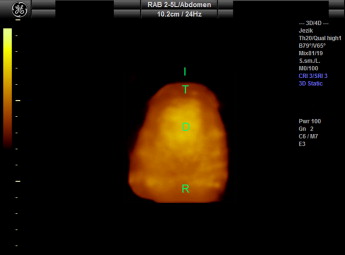
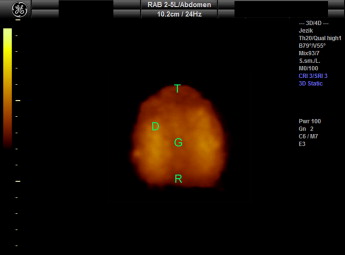
The characteristic 3D reconstruction of the tongue postured on the palate displays distinctive convexity of the tongue dorsum, whereas, in the 3D reconstruction with the tongue postured on the mouth floor, the dorsum is characterized by a central groove and expressed concavity. Posture on the mouth floor was demonstrated by 81.5% of the children with unilateral posterior crossbite and by only 34.8% of those with normal deciduous dentition. The difference was statistically significant (Fisher exact test: P = 0.0012).
Conclusions
Three-dimensional ultrasonography enables objective assessment of tongue posture and could become in the future an important part of functional diagnostics before, during, and after orthodontic treatment.
Unilateral posterior crossbite is one of the most prevalent malocclusions in the deciduous and early mixed dentition and occurs in 4% to 23% of children. Untreated unilateral posterior crossbite is an important risk factor for the development of craniofacial deformities and skeletal orofacial asymmetries. The etiology of this malocclusion can be in general assigned to environmental influences. The most frequent cause for the formation of unilateral posterior crossbite is the reduction in the width of the maxillary arch compared with the mandibular arch as a result of sucking habits, mouth breathing and incompetent lip seal, and visceral type of swallowing with incorrect tongue posture on the mouth floor.
Tongue size, posture, and function are of crucial importance in the etiology of malocclusions and dentofacial deformities. The tongue is the most powerful muscle in direct contact with both dental arches and both jaws, and is therefore one of the most important force sources in this area. Tongue posture is supposed to be even more important than tongue function, since the total time of swallowing is too short to affect the equilibrium of forces on teeth and bones.
Clinical examination of tongue function and posture is limited because of anatomic structures surrounding the tongue, and the evaluation is highly subjective. Many studies have investigated tongue function during swallowing and speech by using radiocinematography, electropalatography, electromagnetic articulography, magnetic resonance, and 2-dimensional ultrasonography. Tongue posture has been evaluated by using lateral cephalograms and computed tomography. The disadvantage of both diagnostic procedures is radiation exposure, which contraindicates these methods in children and disables frequent repetitions of the procedures. In the past decade, ultrasonography was also used, but tongue surface imaging with 2-dimensional ultrasonography is a complicated and unreliable method. Three-dimensional (3D) ultrasound has been used in only 2 studies of partially resected tongues, but there are no data about 3D surface morphology of anatomically normal but diversely postured tongues at rest.
Therefore, the aim of our study was to obtain 3D ultrasound reconstructions of differently postured tongues to evaluate and compare tongue posture in children with unilateral posterior crossbite and those with normal deciduous dentition.
Material and methods
The study was divided into 2 stages. In the first stage, the referential 3D ultrasound reconstructions of the tongues with known postures in adults were obtained; in the second stage, these reconstructions were used as references to assess tongue postures in children with unilateral posterior crossbite and children with normal deciduous dentition. Ultrasound diagnostics were performed by an experienced specialist in radiology (M.K.) trained in the use of 3D ultrasonography. The research was approved by the Ethics Committee, Faculty of Medicine, University of Ljubljana, Slovenia, and the parents were asked to give informed consent to participate in the study.
For the acquisition and reconstruction of the referential 3D ultrasound images, 10 adults (5 men, 5 women) without malocclusion, aged 25.4 ± 0.6 years, were examined in the first part of the study. An ultrasound system Voluson 730 Expert (General Electrics Healthcare, Kretztechnik, Zipf, Austria), and a 3D convex transducer (RAB 2-5 MHz, General Electrics Healthcare) were used in the study. The head of each subject was immobilized in a dental chair with a strap, with the Frankfort horizontal line parallel to the floor. The 3D transducer was coated with aqueous contact transmission gel and positioned at the midsagittal line of the skin of the mouth floor. Each subject was asked to raise her or his tongue to the palate and remain still for 15 seconds. Then the recording procedure was started using the following parameters: 55° to 65° view; mechanical index, 0.8; and thermic index, 0.3. Afterward, each subject was asked to position her or his tongue on the mouth floor, and the procedure was repeated. The acquired data were transferred to a personal computer, and 3D reconstructions were made using the program 4D View (version 5.0, General Electrics Healthcare, Waukesha, Wis).
The next steps were acquisition, reconstruction, analysis of 3D ultrasound images in children with unilateral posterior crossbite and those with normal deciduous dentition, and statistical analysis. Twenty-seven children (12 boys, 15 girls) with unilateral posterior crossbite, aged 3.4 to 6.8 years (mean age, 5.4 ± 1 years) and 23 randomly selected children (13 boys, 10 girls) without morphologic malocclusion or with mild malocclusion according to the morphologic trait of the Eismann-Farčnik index aged 5.7 to 6.8 years (mean age, 6.2 ± 0.4 years) from the local kindergarten and school were examined. As in first part of the study, the head of each child was immobilized in a dental chair with the Frankfort horizontal line parallel to the floor. The transducer was coated with aqueous contact transmission gel and positioned at the midsagittal line of the skin of the mouth floor. Each child was asked to relax and remain still for 15 seconds. No instructions were given for tongue posture. The recording procedure, with the same parameters as in the first part of the research, was repeated twice. The acquired data were transferred to a personal computer, and 3D reconstructions were made by using the same program. Referential 3D reconstructions were then used to asses the tongue posture for each child. The data were analyzed by using the statistical program SPSS for Windows (version 15.0, SPSS, Chicago Ill). The data from both groups of children were compared by using the Fisher exact test, and the statistical significance was predetermined at P <0.05.
Results
The characteristic 3D reconstruction of the tongue postured on the palate is shown in Figure 1 . The tongue dorsum displays distinctive convexity. Figure 2 presents the characteristic 3D ultrasound picture of the tongue surface with the tongue postured on the mouth floor. The tongue dorsum is characterized by a central groove and expressed concavity.
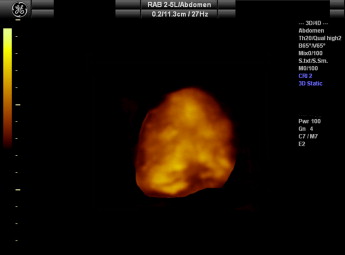
Of the children with unilateral posterior crossbite, 81.5% had ultrasonographically assessed tongue posture on the mouth floor. In the group of children with normal deciduous dentition, 34.8% were found to have the tongue posture on the mouth floor. The result was statistically significant (Fisher exact test: P = 0.0012). In 2 children with unilateral posterior crossbite and in 2 children with normal deciduous dentition, the tongue posture was not constant and demonstrated both postures. Figures 3 and 4 show the surfaces of differently postured tongues in 2 children with unilateral posterior crossbite.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


