Introduction
The purpose of this descriptive study was to estimate retainer wear and compliance among orthodontic patients in the first 2 years after active orthodontic treatment.
Methods
A random sample of 1200 orthodontic patients was selected from 4 offices. Data were collected by a self-administered questionnaire that consisted of 6 items: type of retainer prescribed, age, sex, length of time since debond, and hours per day and nights per week that patients wore their retainers. Responses were solicited by mail or the Internet. Data were gathered on a categorical scale and analyzed.
Results
The overall response rate was 36% during a 6-week period. In the first 3 months after debond, 60% of patients were wearing their retainers more than 10 hours during a 24-hour cycle, and 69% were wearing the retainers every night. At 19 to 24 months after debond, 19% of the patients were not wearing their retainers, and 81% wore their retainers at least 1 night per week. Compliance rates during the periods of 0 to 3, 4 to 6, 7 to 9, 10 to 12, 13 to 18, and 19 to 24 months were 69%, 76%, 55%, 62%, 45%, and 45%, respectively. Age, sex, and type of retainer did not influence the levels of compliance.
Conclusions
Most continued to wear their retainers at least 1 night per week, with compliance rates, as defined, tending to decrease in our sample. It was encouraging that 81% of the patients in this sample largely maintained their orthodontic result.
Retention of orthodontic results is a critical component for successful long-term treatment. The retention phase almost entirely depends on the patient, since most orthodontists prescribe removable appliances. A national study of 2000 orthodontists by Valiathan and Hughes showed that most orthodontists prescribe less than 9 months of full-time wear of removable retainers and thereafter advise part-time, but lifelong wear. They also reported that a greater percentage of orthodontists prescribing Hawley retainers recommend longer full-time wear (3-9 months) compared to clear thermoplastic retainers (3 months or less). The most common part-time wear schedule was 8 hours a day, and 84% of orthodontists who prescribed removable retainers recommended lifetime retainer wear. Although we may now better understand the prescriptions most commonly advised by our colleagues, are patients complying with retainer wear and can we predict their behavior?
Hichens et al performed a randomized, controlled, clinical trial in 1 orthodontist’s office to evaluate patient satisfaction between the Hawley and the vacuum-formed retainer (VFR). The study included 201 patients receiving VFRs and 196 receiving Hawley retainers. Patients were instructed to wear both the VFRs and Hawley retainers 24 hours a day for the first 3 months and 12 hours per day from 3 to 6 months after treatment. Most subjects preferred VFRs, with 85% of the Hawley group and 95% of the VFR group stating that they were wearing the retainers over the 6-month time period. The study was not designed to test compliance and did not indicate the amount of time the retainers were used per day or week.
When we assessed compliance from the orthodontic literature, some studies found age to be related, but others did not, with compliance rates typically decreasing with age. Similarly, studies reported that girls were more compliant than boys, but others found no difference. In the medical literature on patient behavior, it is not uncommon to find that a third of patients never comply with their medications, regardless of whether they were advised about long-term oral penicillin use for rheumatic fever in children or antihypertensive drugs in steelworkers.
Orthodontic retention is a complex issue. The age of the patient, retainer design, parental influence, orthodontist’s prescription, and fear or disregard of relapse are all factors that are likely to influence patient behavior. Changes in parental influence, in either promoting adaptive behaviors or providing standards against which to rebel, along with increasing importance of peers and developmental issues related to emerging adult identity, might encourage resistance in some and greater maturity in others to follow the health care recommendations.
The purpose of our descriptive study was to identify patient behaviors pertaining to the use of their retainers. Specifically, we attempted to estimate the number of hours per day and week that patients wore their retainers in the first 2 years after active orthodontic treatment, and whether that agreed with the prescription advised by their orthodontists.
Material and methods
The procedures and protocols for this study were approved by the Institutional Review Board at Case Western Reserve University, Cleveland, Ohio. After we critically reviewed the literature, our initial survey instrument was designed with the “tailored design method.” The questionnaire was pilot tested on 11 retention patients in the Department of Orthodontics. The responses were reviewed, and minor revisions were made to form a preliminary survey instrument. The preliminary survey was converted to electronic form and hosted on SurveyMonkey.com . The electronic version was once again tested on 11 different patients and revised as needed to arrive at the final survey instrument. The final survey consisted of 6 questions, 4 to characterize our sample and 2 to help identify how long retainers were worn in the first 2 years after active treatment.
Four private orthodontic offices in the area consented to participate in the study. The questionnaire, with a cover letter explaining the purpose of the study, was mailed along with a postage-paid self-addressed envelope to 1200 randomly selected patients, from 4 separate orthodontic offices. All patients had their orthodontic braces removed between January 15, 2006, and January 15, 2008. The offices were selected based on their respective retention protocols, in an effort to best match their protocols with the most commonly prescribed retention protocols in the United States. The number of patients debonded in the last 2 years in the 4 offices, and the common retention protocols prescribed, were the following.
-
Office 1: 663 patients; maxillary and mandibular VFRs prescribed 24 hours a day for 6 weeks, 12 hours for the next 3 months, followed by nighttime wear starting from 4.5 months for the remaining 19.5 months.
-
Office 2: 1015 patients; maxillary VFR and Hawley (patient chooses which to wear) with fixed mandibular 3-3, prescribed 24-hour wear for 3 months, with nighttime wear from 4 to 24 months.
-
Office 3: 582 patients; maxillary VFR with mandibular fixed 3-3, prescribed 10 to 15 hour wear for 3 months, with nighttime wear from 4 to 24 months.
-
Office 4: 387 patients; maxillary VFR for the first 2 weeks followed by a maxillary Hawley and mandibular fixed 3-3, prescribed 24-hour wear for 6 months with nighttime wear from 7 to 24 months.
All offices instructed the patients about continued nighttime wear for life when they were dismissed as retention patients after 2 years of observation.
To obtain statistical significance, 370 responses were required; the estimate was based on the total of 2638 patients, a 95% confidence interval, and a 5% sampling error. No patients debonded during the stipulated time frame were excluded, giving all patients an equal opportunity to participate. Since we expected a 33% response rate, we randomly selected 300 patients from each office, for a total of 1200. Surveys were mailed to each patient from the respective orthodontist’s office according to the approved protocols. The envelopes contained a cover letter from the orthodontist, a 1-page letter from the investigators describing the project, the 2-page survey, and a postage-paid, self-addressed envelope. Participants were also given the option of completing the survey online by providing them a link and unique identification number in the survey they received. The time frame to collect responses was 6 weeks from the date of mailing.
After 6 weeks, hard-copy responses were manually entered, and Internet responses were recorded as categorical data by using Microsoft Excel 2007 spreadsheets (Microsoft, Redmond, Wash). Partially completed responses were excluded. Response rate was calculated as the number of surveys returned divided by the number of surveys that were sent out and not returned as undeliverable. The overall response rate was 36.1%, and the effective response rate was 35.7%. Five surveys were excluded due to incongruent answers. In all, 2598 individual responses were entered into the spreadsheet, and 33 mistakes were corrected after manual double data entry, representing .012% of responses. For reliability, double data entry was performed by manually entering age, sex, and length of time since debond from the responding patients’ treatment files into a separate spreadsheet. This secondary spreadsheet was cross-referenced with the initial spreadsheet to evaluate reliability. Any errors were further assessed, recorded, and manually corrected. SPSS software (version 16, SPSS, Chicago, Ill) was used to calculate frequencies and percentages, and to run chi-square tests to detect differences between offices. The chi-square tests assessed the differences in compliance levels among the 4 offices and the following variables: age, sex, type of retainer, and length of time since debond. Compliance was determined by adherence to the “lowest common denominator” among the office retention protocols. Individual compliance rates during each period (0-3 to 19-24 months) were combined to create 1 overall compliance or noncompliance level on a dichotomous scale, which was then used in a logistic regression. The logistic regression was performed with noncompliance as the dependent variable and the offices, type of retainers, sex, and lengths of time since debond, the independent variables. The significance level (alpha) for the chi-square tests and logistic regression analyses were set at ≤0.05.
Results
During the 6 weeks of data collection, 428 (36% overall) completed surveys were received of the 1200 mailed surveys. The response rate from the offices ranged from 31.0% to 40.7%. Only 10% of the respondents were in the age 13 and younger category; the majority (24.8%) were 15-year-olds. We received 110 (36.7%), 93 (31.0%), 122 (40.7%), and 103 responses (34.3%) from offices 1 through 4, respectively. Of the 428 respondents, 396 chose to complete the paper survey mailed to them, and 32 chose the web-based survey. Six surveys were excluded from the final results: 5 paper surveys due to incongruent answers, and 1 web-based survey because the identification number was incorrect. Sixty percent of respondents were female, and 40% male. Table I describes the characteristics of our sample: age, sex, length of time since debond, type of maxillary and mandibular retainers, and numbers of responses from each office. The range of responses for length of time since debond was 12% to 22%, with the least responses in the 7-9 months category, and the largest coming from the 19-24 months category. The most common removable retainers in both the maxilla and the mandible were VFRs: 66.4% and 28%, respectively.
| Variable | n | Percent |
|---|---|---|
| Respondents of 300 surveys sent to | ||
| Office 1 | 110 | 36.7% |
| Office 2 | 93 | 31.0% |
| Office 3 | 122 | 40.7% |
| Office 4 | 103 | 34.3% |
| Age (y) | ||
| ≤13 | 42 | 9.8% |
| 14 | 53 | 12.4% |
| 15 | 106 | 24.8% |
| 16 | 75 | 17.5% |
| 17 | 66 | 15.4% |
| ≥18 | 86 | 20.1% |
| Length of time since debond (mo) | ||
| 0-3 | 75 | 17.5% |
| 4-6 | 70 | 16.4% |
| 7-9 | 51 | 11.9% |
| 10-12 | 53 | 12.4% |
| 13-18 | 85 | 19.9% |
| 19-24 | 94 | 22.0% |
| Maxillary retainer type | ||
| VFR | 284 | 66.4% |
| Hawley | 138 | 32.2% |
| Bonded | 1 | .2% |
| Other | 5 | 1.2% |
| Mandibular retainer type | ||
| VFR | 120 | 28.0% |
| Hawley | 14 | 3.3% |
| Bonded | 271 | 63.3% |
| Other | 23 | 5.4% |
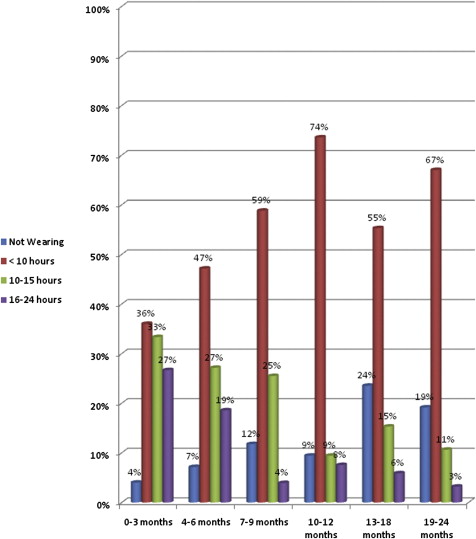
Figures 1 and 2 represent the hours per day and nights per week that the patients wore their retainers compared with length of time since debond. In the first 3 months after treatment, 27% of the patients wore their retainers 16 to 24 hours, 36% wore them less than 10 hours per day, and 4% did not wear them at all. From 19 to 24 months after debond, 19% were not wearing retainers at all during the day, 67% were wearing them less than 10 hours, and 11% were still wearing the retainers 10 to 15 hours.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


