Introduction
This was a prospective randomized clinical trial comparing the effect of bracket type on the duration of orthodontic treatment and the occlusal outcome as measured by the peer assessment rating (PAR).
Methods
A multi-center randomized clinical trial was carried out in 2 orthodontic clinics. Sixty-two subjects (32 male, 30 female; mean age, 16.27 years) with a mean pretreatment PAR score of 39.40, mandibular irregularity from 5 to 12 mm, and prescribed extractions including mandibular first premolars were randomly allocated to treatment with either the Damon3 self-ligated or the Synthesis conventional ligated preadjusted bracket systems (both, Ormco, Glendora, Calif). An identical archwire sequence was used in both groups excluding the finishing archwires: 0.014-in, 0.014 × 0.025-in, and 0.018 × 0.025-in copper-nickel-titanium aligning archwires, followed by 0.019 × 0.025-in stainless steel working archwires. Data collected at the start of treatment and after appliance removal included dental study casts, total duration of treatment, number of visits, number of emergency visits and breakages during treatment, and number of failed appointments.
Results
Sixty-two patients were recruited at the start of treatment, and the records of 48 patients were analyzed after appliance removal. Accounting for pretreatment and in-treatment covariates, bracket type had no effect on overall treatment duration, number of visits, or overall percentage of reduction in PAR scores. Time spent in space closure had an effect on treatment duration, and the pretreatment PAR score influenced only the reduction in PAR as a result of treatment.
Conclusions
Use of the Damon3 bracket does not reduce overall treatment time or total number of visits, or result in a better occlusal outcome when compared with conventional ligated brackets in the treatment of extraction patients with crowding.
In the last decade, there has been a significant increase in the number of self-ligated bracket systems available to orthodontists. Currently, 1 market leader is the Damon system (Ormco, Glendora, Calif), which advocates a treatment philosophy based on the use of a passive self-ligated bracket design and superelastic nickel-titanium archwires. According to proponents of this system, the low-force and low-friction environment provided by the Damon appliance offers considerable advantages over those with conventional ligation. These include greater patient comfort during treatment, fewer visits to the orthodontist, shorter overall treatment times, less need for extractions, and better outcomes in terms of both occlusal and facial esthetics.
To date, these claims have been based on theoretical arguments, isolated case reports, case series, and retrospective comparisons. Although attempts have been made to achieve equivalence between samples compared retrospectively, some studies have suffered from poor design, inadequate reporting, and significant bias. In an attempt to improve the evidence base relating to the Damon system, several prospective randomized clinical trials have been instigated. Some of these have compared pain and discomfort caused by several Damon bracket designs and conventional ligation during the initial alignment phase of treatment and, collectively, have shown that the Damon system is not associated with any significant reductions in pain and discomfort compared with conventional appliances. They have also reported on the rate of initial tooth alignment, where there is weak evidence that Damon2 brackets can resolve mild crowding more rapidly than conventional appliances when this treatment is carried out on a nonextraction basis. However, for more severe crowding treated with the Damon3 bracket and first premolar extractions, this is not the case. In addition, the Damon MX passive self-ligated bracket cannot resolve maxillary anterior crowding any more effectively than an In-Ovation R with active self-ligation. Collectively, these studies have also demonstrated that the Damon appliance does not align teeth in a qualitatively different manner from conventional or active self-ligated appliances; incisor proclination and canine expansion occur just as readily with the Damon system as they do with conventional ligated preadjusted brackets. Although the literature relating to the clinical use of self-ligated bracket systems is relatively new, currently little objective evidence suggests that they offer significant advantages with regard to treatment efficiency when compared with conventional appliances.
However, the period of initial alignment contributes toward only 1 part of the overall treatment time, which in total depends on many other factors. These can be patient-based, such as age, severity of the underlying malocclusion, and compliance, or treatment-based, including factors such as the decision to extract teeth, the need for overbite reduction, and space closure. Therefore, for any investigation of overall treatment effectiveness, it is important to evaluate this over the entire duration, from appliance placement to removal on completion. Moreover, for a sample with pretreatment equivalence, the duration of treatment is relevant only when evaluated in relation to outcome. Treatment outcome can be assessed in many ways, but one of the most recognized is the peer assessment rating (PAR), which provides a validated numeric score based on several occlusal features before and after treatment. The difference in these scores gives an indication of improvement in treatment and whether the occlusal aims were achieved.
The aim of this randomized clinical trial was to compare the efficiency of treatment by using Damon3 self-ligated and conventional bracket systems in terms of overall treatment time, number of visits, and occlusal outcome, as measured by the PAR index.
Material and methods
Detailed descriptions of the methodology used for this study have been previously reported. Ethical approval was obtained from the Research Ethics Committee (no: 04/Q0704/116) of Guy’s Hospital in London, United Kingdom, and written consent was obtained from all parents or guardians and children. The subjects were recruited from a sample of consecutive patients attending the orthodontic departments at Kings College London Dental Institute and Kent and Canterbury Hospital who satisfied the following criteria: (1) under 30 years of age at the start of treatment, (2) no medical contraindications, (3) permanent dentition, (4) mandibular incisor irregularity between 5 and 12 mm, (5) extraction of the mandibular first premolars as part of the normal treatment plan, and (6) absence of a complete overbite.
After we obtained consent, the subjects were randomly allocated for treatment with either the Damon3 passive self-ligated bracket or the Synthesis conventional ligated preadjusted edgewise bracket (both, Ormco) by using a restricted random number table to ensure equivalence of numbers in each group. The bonding method was standardized between the groups, by using conventional etching and BluGloo bracket adhesive (Ormco) according to the manufacturer’s instructions. Mandibular dental study casts were taken at appliance placement (T1). After bracket bonding, Damon 0.014-in copper-nickel-titanium archwires were placed and ligated to all teeth by using the self-ligation system for Damon3 or standard elastomeric ligatures for Synthesis. The subjects were reviewed at approximately 6 to 8 week intervals, and a sequence of 0.014 × 0.025-in and 0.018 × 0.025-in copper-nickel-titanium, followed by 0.019 × 0.025-in stainless steel archwires, was used. On placement of the 0.014 × 0.025-in copper-nickel-titanium archwire, a further mandibular dental study cast was taken (T2). Treatment continued, and another mandibular study cast was taken at the end of alignment (T3). Treatment was then continued to completion, as judged ultimately by 2 orthodontic operators (A.T.D. and M.T.C.), and active treatment was recorded as completed on the day of appliance removal. A final set of dental study casts were taken at this point (T4).
For inclusion in the final analysis of treatment outcome at T4, the subjects had to fulfill the following criteria: (1) all records complete, (2) no more than 3 unexplained failed appointments during active treatment, and (3) treatment without orthognathic surgery. Data collection included the total duration of active treatment with fixed appliances, the number of visits (including emergency appointments), before and after PAR scores as recorded from the dental study casts, and the overall improvement in PAR score as a percentage.
Statistical analysis
SPSS software (version 13.0, SPSS for Windows, Chicago, Ill) was used for descriptive and statistical analysis with analysis of covariance (ANCOVA) to compare the treatment effect of the bracket systems while accounting for baseline differences and confounding continuous variables. These included the age of the patient, the initial PAR score, whether ectopic maxillary canines were mechanically erupted during treatment, the number of failed appointments, and the number of breakages during treatment. The level of statistical significance was set at P <0.05. In our initial analysis to determine the effect of sex on treatment duration, we found no statistically significant effect (F ratio 0.057, P = 0.813), so further analysis was carried out without discrimination for sex.
Results
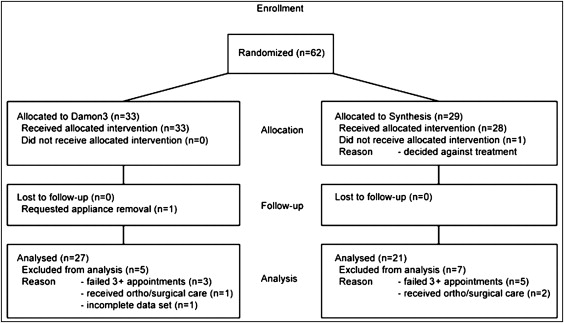
Sixty-two patients were recruited to the original study, with 33 (mean age, 16.19 years; SD, 3.68) allocated to treatment with the Damon3 bracket and 29 (mean age, 16.38 years; SD, 5.28) to the Synthesis. The flow of patients through the study and the reasons for excluding patients from the final data set are shown in the Figure . From this original sample, 48 were included in the final analysis at T4 ( Table I ). In this sample, the range of malocclusions treated by using the 2 appliance systems was broadly similar, except that there were no Class III patients in the Synthesis bracket sample ( Table I ).
| Damon3 | Synthesis | Total sample | |
|---|---|---|---|
| Number randomized | 33 | 29 | 62 |
| Sample group at T4 | 27 | 21 | 48 |
| Class I | 7 (15%) | 6 (13%) | 13 (28%) |
| Class II | |||
| Division 1 | 14 (29%) | 13 (27%) | 27 (56%) |
| Division 2 | 2 (4%) | 2 (4%) | 4 (8%) |
| Class III | 4 (8%) | 0 | 4 (8%) |
| Maxillary anchorage support | 10 (21%) | 9 (19%) | 19 (40%) |
| Maxillary ectopic canines | 2 (4%) | 2 (4%) | 4 (8%) |
Descriptive statistics for the 2 groups are shown in Table II , including overall treatment times, total numbers of visits (including emergency appointments), pretreatment and posttreatment PAR scores, and the overall percentages of reduction in PAR scores.
| Damon3 | Synthesis | Total sample | |
|---|---|---|---|
| Treatment duration (mo) | 24.48 (6.72) | 23.00 (4.86) | 23.83 (5.96) |
| Visits (n) | 14.22 (2.64) | 14.48 (3.53) | 14.33 (3.03) |
| Breakages (n) | 2.74 (2.41) | 2.29 (2.74) | |
| Pretreatment PAR | 38.26 (9.91) | 40.86 (9.38) | 39.40 (9.66) |
| Posttreatment PAR | 5.48 (3.62) | 6.43 (3.76) | 5.90 (3.67) |
| PAR reduction (%) | 85.19 (8.99) | 83.38 (9.41) | 84.40 (9.12) |
Analytic statistics for the 2 groups are shown in Table III . Analysis consisted of ANCOVA to test for differences in means between the 2 groups but accounting for pretreatment factors, including age at T1, the pretreatment PAR score, and confounding variables during treatment, including the number ectopic maxillary canines mechanically erupted , the number of failed appointments, duration of space closure, and the number of breakages. When these factors were covaried out, the effect of the bracket system used on total duration of treatment (F ratio = 0.000; P = 0.992) and number of visits (F ratio = 0.956; P = 0.334) was not significant. In contrast, the duration of space closure had a significant effect on the duration of treatment ( P = 0.036) but not on the number of visits ( P = 0.284). When the pretreatment PAR score was covaried out, the effect of the bracket system on total PAR reduction (F ratio = 1.046; P = 0.312) was not significant. The pretreatment PAR score, however, had a significant effect on total PAR reduction ( P = 0.022).


