Fig. 7.1
(a, b) Lips are important for the smile design as they frame of the mouth. Upper lip is especially important in the smile design process, as it reveals the visible amount of teeth and gingiva while the lips are at rest and smiling
Fig. 7.2
(a–c) Evaluating the incisal edge position at rest and smiling is important for further oral esthetics
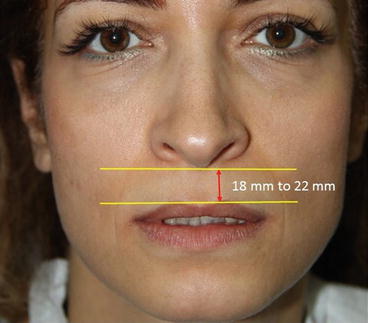
Fig. 7.3
Lip length can differ depending of gender, measuring for male patients around 22 ± 2 mm and for females around 20 ± 2 mm
Fig. 7.4
Patients’ age and tooth wear can affect the visibility of tooth structure at rest. (a) Visibility of tooth structure at rest for a 20-year-old patient. (b) Visibility of tooth structures at rest for a 50-year-old patient
Fig. 7.5
In general the upper lip is wider and longer than the lower lip where the teeth are properly aligned compared with the lower lip

Fig. 7.6
Lip mobility or movement of the upper lip is an important determinant for exposure of the teeth and gingival structures
7.1 Incisal Edge Position
Incisal edge position refers to the visible tooth structure when the lips are at rest (Figs. 7.2b and 7.4a, b) [1, 5], and varies depending on age and sex [1, 2, 4, 5, 9, 10]. Besides age and gender of the patient, evaluation of the upper lip length and curvature help to determine the incisal edge length [5]. There are conflicting reports in the literature regarding the incisal edge position of the maxillary centrals [1–5, 9–11], although most authors report that an average visible tooth structure of 2–4 mm when the lips are at rest is esthetically pleasing [2, 3, 10–13]. In younger patients (Fig. 7.4a) the visible tooth structure tends to be more extensive than in older patients (Figs. 7.2b and 7.4b), and it has been reported that this can vary depending on ethnicity [6, 13, 14]. While a younger female patient around 20 years of age displays 3–5 mm of maxillary incisal edge at rest with no visible mandibular teeth [5], a male patient of the same age can display 1–2 mm less incisal edge [14]. In addition, aging leads to a diminution in muscle tonus and occurrence of tooth wear, and the visible maxillary incisal edge decreases; for instance, a 45–50-year-old male patient may not show any maxillary incisal edge at rest, whereas a woman of the same age may display a slight amount [13, 14] (approximately 1–1.5 mm) [2] while the amount of mandibular incisal display increases [1, 5, 13]. Therefore, in creating an esthetically pleasing and youthful smile, the amount of maxillary central incisal edge on display is an important factor in smile design procedure [1]. Another important guide for evaluation of incisal edge position of the maxillary anterior teeth and creation of an ideal smile is that while smiling, the incisal tips of the maxillary canines should slightly touch (Fig. 7.7a) or come fairly close to the lower lip (Fig. 7.7b), and in the same position the maxillary incisors should be approximately 2–3 mm away from touching the lower lip [10, 12, 15]. However, curvature of the lower lip can affect the achievement of this ideal smile position [10, 15]. During smiling, maxillary premolars normally are displayed in the frame of the lips, and in some patients with longer lips the first molars can also be displayed.

Fig. 7.7
For creation of an ideal smile, incisal tip of the maxillary canines (a) should slightly touch the lower lip or (b) come fairly close to the lower lip during smiling
If during clinical examination insufficient or too much tooth display is observed during smiling, the clinician must determine the tooth length and position. If maxillary incisal edge display at rest position is less than 3–4 mm (Fig. 7.4b), lengthening of incisal edge of the teeth by composite addition should be considered [10, 12]. Clinician can observe the changes on the patient’s face and communicate with the patient on the proposed changes by using temporary resins for this purpose (Fig. 7.8) [10]. If maxillary incisal edge display is normal (3–4 mm) at rest and the length of the crowns are visualized as too short, the clinician must consider a crown-lengthening procedure to achieve normal tooth length [10]. Before the crown-lengthening procedure, proposed changes on the gingival tissue and teeth can be shown to the patient by adding composite resin over the current gingival margin.

Fig. 7.8
Patient exhibiting less than 3–4 mm maxillary incisal edge display at rest (Fig. 7.4b), and incisal lengthening by adding temporary acrylic resin in to the incisal edge of the teeth using silicone matrices prepared form diagnostic wax-up model
To help determine the correct incisal edge position at rest, the clinician can use phonetic guidelines by repeating several letters [1, 2, 4, 5]. While sitting in the postural head or upright position the patient is asked repeatedly pronounce the letter “M” and keep the lips relaxed, whereby the clinician can determine the incisal edge position of the maxillary central teeth at this resting position (Fig. 7.9) [2, 3, 5, 11]. After this repeated pronunciation is interrupted, the upper and lower lips return easily to the relaxed position for assessment [5]. In this position the clinician can examine the amount of visible maxillary and mandibular teeth at the incisal edge, which can differ according to the age of the patient [11]. By this phonetic examination the clinician may consider crown lengthening either apically or incisal, according to the visible tooth structure at rest, while preserving the width-to-length ratio and paying attention to occlusion [2]. As previously described, the amount of maxillary incisal display depends on the age of patient, tooth wear, and upper lip length, and varies from patient to patient [1, 5, 6, 13, 14].

Fig. 7.9
After repeatedly saying the letter “M” and then keeping the lips at rest allows the clinician to determine the incisal edge position of the maxillary central teeth
Another important phonetic examination in smile analysis is the use of the “E” sound [4, 5, 11, 16]. Pronunciation of “E” by the patient shows widest smile (Fig. 7.10), which allows evaluation of the incisal edge position of the maxillary anteriors and the incisal line [4, 5, 11, 16]. By having patient say “E” without interruption, e.g., “eeeeee” [5] or “cheeeese,” the clinician can examine the incisal edge in this maximum extension position of the lips [11]. Maxillary central incisor edge should come close to the upper border of the lower lip during this examination [16]. For an esthetically pleasing smile, the incisal edge of the maxillary teeth should be positioned halfway between the upper and lower lip during uninterrupted pronunciation of “E” (Fig. 7.11) [4, 5, 11]. Loss of muscle tonus caused by aging and tooth wear can affect the visibility of the teeth during the pronunciation of the extended “E” sound, and results in less or no incisal edge display [13, 14, 16].


Fig. 7.10
Pronunciation of extended “E” sound, such as saying “cheese,” allows the clinician to evaluate the incisal edge position of the maxillary anteriors and the incisal line
Fig. 7.11
Positioning the incisal edge of the maxillary teeth halfway between the upper and lower lip during uninterrupted pronunciation of the letter “E” creates an esthetically pleasing smile
“F” and “V” sounds are also important in determining the maxillary central incisal edge [2, 4, 5, 16]. When the patient correctly pronounces the “F” and “V” sounds, the incisal edge of the maxillary anterior teeth should come in slight contact with the wet-dry line or vermilion border of the lower lip (Fig. 7.12a, b) [2, 4, 5, 16]. By having the patient produce these sounds, the maxillary anterior teeth lightly press on the lower lip and partially block the air passage [5], thus helping to correctly determine the labiolingual position and length of the maxillary anterior teeth [4, 5]. In another approach, correct labiolingual positioning of the maxillary anterior teeth by placing the incisal edges on the wet-dry border of the lower lip allows the patient to correctly pronounce “F” and “V” [5, 17].
Fig. 7.12
Phonetic evaluation of the patient during pronunciation of the “F” sound for determination of incisal edge of the maxillary centrals. (a) Phonetic evaluation with the temporaries. (b) Phonetic evaluation without temporaries
Pronunciation of the “S” sound is also an important parameter in determining the incisal edge of the maxillary centrals and the correct vertical height dimensions [4, 5, 16]. During pronunciation of the “S” sound the mandibular central incisors are positioned 1 mm behind and 1 mm below the maxillary incisal edge, the teeth being slightly in contact (interocclusal position) (Fig. 7.13) [4, 5]. Correct incisal edge position is important, as it is related to the inclination of the maxillary anterior teeth, labial and lingual contours, anterior guidance, and tooth display [4]. Inclination of the maxillary anterior teeth greatly affects the labial and lingual contours, anterior guidance, and incisal edge position. As a result, all these factors have important roles in the esthetic and functional aspects of the final restorations [4]. These clinical guidelines are subjective, and should be used as basic principles to determine appropriate incisal edge positioning of a particular patient [3]. For correct evaluation of the case and a natural, functional, and esthetically pleasing outcome, the clinician also should use composite mock-ups, provisional composite or acrylic restorations, diagnostic wax set-ups, and digital imaging in communication with the patient, multidisciplinary team members, and dental technicians. Composite mock-ups and provisional restorations can be helpful in determining the correct incisal edge position for the final restorations.

Fig. 7.13
Evaluation of the patient during pronunciation of the “S” sound with and without temporaries for determination of incisal edge of the maxillary centrals
7.2 Incisal Display
Position and size of the teeth, lip length, and lip mobility are the most important factors affecting maxillary incisal display [12]. As previously described, lip length differs according to gender and the reference measure from subnasale to the border of the upper lip (Fig. 7.3), and can be measured as between 18 and 24 mm [6, 7, 10, 12]. Under normal smile conditions the average lip mobility has been reported at around 7–8 mm [10, 12]. At rest, the maxillary incisor display should be between 2 and 4 mm, and while smiling all of the maxillary anterior teeth and premolars should be displayed with approximately 1–2 mm gingival exposure [10, 12, 18]. Kokich et al. [19
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


