Introduction
Our objectives were to determine the validity and reproducibility of measurements on stereolithographic models and 3-dimensional digital dental models made with an intraoral scanner.
Methods
Ten dry human skulls were scanned; from the scans, stereolithographic models and digital models were made. Two observers measured transversal distances, mesiodistal tooth widths, and arch segments on the skulls and the stereolithographic and digital models. All measurements were repeated 4 times. Arch length discrepancy and tooth size discrepancy were calculated. Statistical analysis was performed by using paired t tests.
Results
For the measurements on the stereolithographic and digital models, statistically significant differences were found. However, these differences were considered to be clinically insignificant. Digital models had fewer statistically significant differences and generally the smallest duplicate measurement errors compared with the stereolithographic models.
Conclusions
Stereolithographic and digital models made with an intraoral scanner are a valid and reproducible method for measuring distances in a dentition.
Successful treatment planning in dentistry requires precise diagnostic information and an extensive diagnosis. In orthodontics, dental model analysis is an essential part of this process. Dental models can be used to evaluate occlusion and perform measurements more easily and accurately than in the patient’s mouth. Measurements typically made for orthodontic diagnosis are overjet, overbite, tooth sizes, arch lengths, and transversal distances. Space can be analyzed by calculating the arch length discrepancy. Disproportions among sizes of maxillary and mandibular teeth can be defined by using the tooth size discrepancy calculations according to Bolton. For dental model analysis, plaster models have been the standard for years. However, plaster models are subject to loss, fracture, and degradation and require physical storage space. To overcome these disadvantages, 3-dimensional digital dental models are an alternative. Additional advantages of digital models are easy storage and exchange with electronic data transfer. Digital models can be virtually manipulated, precise cross-sectional views can be created, and they can be magnified. Commercially available digital models can be produced by a direct or an indirect method. Indirect methods begin with dental impressions. Digital models can then be obtained by laser scanning of plaster models or computed tomography imaging of the impressions or plaster models. The direct method uses an intraoral scanner to scan directly in the patient’s mouth, making dental impressions redundant. This can be advantageous for patients with a gag reflex or with cleft lip and palate, who are at risk of aspiration and respiratory distress during taking of the dental impressions. Recently, the validity of digital models produced with an indirect method was evaluated in a systematic review by assessing the agreement of measurements on digital and plaster models. It was concluded that digital models offer a high degree of validity, and measurement differences are likely to be clinically acceptable. To our knowledge, no study has assessed the validity of measurements on digital models obtained with a direct method with an intraoral scanner. Therefore, the aim of this study was to determine the validity and reproducibility of orthodontic measurements made on stereolithographic and digital models created with an intraoral scanner.
Material and methods
Ten dry human skulls were selected from the files of the Department of Orthodontics and Craniofacial Biology at Radboud University Medical Centre, Nijmegen, The Netherlands. The inclusion criteria were (1) full permanent dentition from the left first molar to the right first molar in both jaws, with 1 missing or deciduous tooth per skull accepted, and (2) dentition without abnormal morphology, with defects of teeth accepted when they did not affect the mesiodistal or buccolingual diameter of the crown.
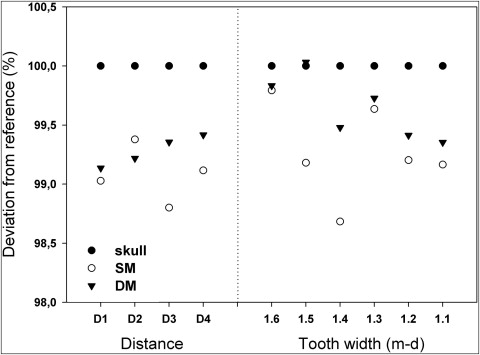
The dentitions were scanned with a chair-side oral scanner (Lava, 3M ESPE, Seefeld, Germany) according to the manufacturer’s manual to create stereolithographic files. After scanning, the files of the scanner were sent to the company by e-mail. This company uses a computer program to correct for missing data, and the files were returned to our university by the Internet. These files were then transformed into digital models by software (OrthoProof, Nieuwegein, The Netherlands). A dental laboratory (Oosterwijk, Utrecht, The Netherlands) used the same files to produce stereolithographic models with a 3-dimensional printer, made from epoxy resin. An example of the 3 models used in this study is shown in Figure 1 .
Two experienced observers (A.M.R.C. and M.C.H.) measured the dentitions on the skulls on the stereolithographic and digital models. A digital caliper (Mauser, Winterthur, Switzerland) was used for the measurements on the dentition and the stereolithographic models. The beaks of the digital caliper were sharpened to a fine edge to improve measurement accuracy. All measurements on the digital models were made by using the software program DigiModel (version 2.3.6; OrthoProof). The digital models could be rotated, magnified, and sliced during measuring. The computer screens used were 15.4 in, with a screen resolution of 1280 × 800 pixels and 32-bit color. The observers repeated all measurements 4 times with a minimum interval between repetitions of a week.
The following measurements were made on the skulls and the stereolithographic and digital models: intermolar distances, intercanine distances, mesiodistal tooth widths, and dental arch segments. There were recorded to the nearest 0.01 mm. The definitions of these measurements are given in the Table .
| Measurement | Definition |
|---|---|
| Intermolar distance | Transversal distance between the mesiobuccal cusp tips of the first permanent molars |
| Intercanine distance | Transversal distance between the crown tips of the permanent canines |
| Mesiodistal tooth width | Greatest mesiodistal diameter measured perpendicular to the axis of the tooth |
| Dental arch segments | Segments were measured by using estimated contact points in a nicely aligned dental arch:
|
All measurements were made in both arches, and the mesiodistal widths were measured for all incisors, canines, premolars, and first molars. The arch length discrepancy, and the anterior Bolton and overall Bolton ratios were calculated.
Statistical analysis
For all models, both means and duplicate measurement errors of all distances were compared by using paired t tests. This was done for both observers separately and combined. The level of significance was set at P ≤0.05.
The mean measurements on the skulls were used as the standard values. Mean differences in measurements between skulls and either stereographic or digital models are informative but do not reveal how often a relatively large deviation from the standard values occurred. Therefore, a large deviation was counted by using arbitrarily chosen cutoffs: 0.1 mm for mesiodistal widths, 0.2 mm for segments, 1.0 mm for transversal distances and arch length discrepancies, and 1.5 mm for tooth size discrepancies. Deviations larger than the cutoffs were compared by using the Fisher exact test version of the chi-square test.
Results
The reproducibility of the measurements was tested. At only 3 times, a significant difference was found, but this difference was not statistically significant. The correlation coefficients of the absolute measurements were high (mean, 0.986; range, 0.876-0.999). We concluded that the outcome of the measurement is independent of the method and the observer. Therefore, only pooled comparisons are presented.
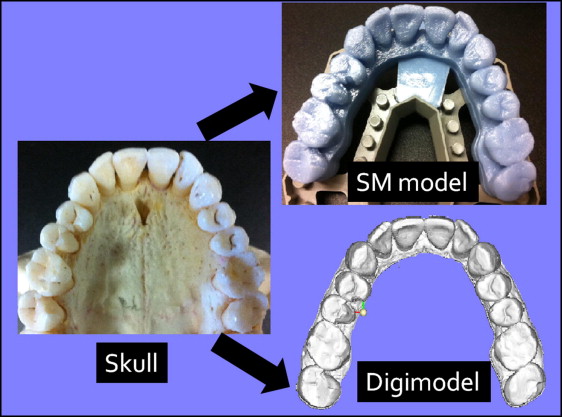
The mean values for dental measurements, arch length discrepancies, and tooth size discrepancies on the skulls and the stereolithographic and digital models were compared with the paired t test. Of the 44 variables, 37 showed statistically significant differences between the skulls and the stereolithographic models. All of these differences showed greater distances on the skulls than on the stereolithographic models, except for segments 33 and 43 and the arch length discrepancy. Fifteen statistically significant differences were found between the measurements on the skulls and the digital models. In these 15 cases, the distances measured on skulls were greater, except for segment 33 and the arch length discrepancy. When the measurements on the stereolithographic and digital models were compared, in 26 cases, statistically significant differences were seen. In all cases (except for arch length discrepancy), greater values on the digital models than on the stereolithographic models were found. An example of the deviation of the distances and measurements of the dentition in the first quadrant is shown in Figure 2 .