Fig. 8.1
Maxillary central incisors are the key element as they are the dominant teeth in the smile

Fig. 8.2
Median or polydiastemas may cause anterior esthetic concerns for the patients due to altered tooth size, proportions, and sometimes morphology
8.1 Tooth Size
Before initiation of any esthetic restorative treatment procedure, the clinician should determine interdental spacing and tooth size by using an appropriate instrument such as a caliper (Fig. 8.3). Maxillary central incisors are the most dominant teeth in an esthetic restorative treatment procedure, therefore, the clinician can primarily begin with the measurement of these teeth to correct median and/or polydiastemas. In addition, a detailed analysis can be performed by the orthodontist using “Bolton analysis,” which compares the overall tooth measurements in one arch relative to the other (please see below) [3].

Fig. 8.3
Determination of maxillary central incisor size using a digital caliper
Creating an ideal single tooth proportion is essential in diastema correction since imbalance in the restored tooth proportion may occur after diastema closure [4]. Single tooth proportion is defined by the ratio of width to length of a tooth. A pleasing and natural width to length tooth ratio is therefore important for creating an esthetically pleasing final outcome in diastema closure. It has been reported previously that a pleasing tooth proportion for maxillary central incisor should be 80 % within the acceptable esthetic range of 75–85 % (Fig. 8.4) [2, 4]. Increasing or decreasing these proportions would produce square or rectangular form (Fig. 8.5) for a single tooth and would create an unaesthetic appearance. Changes in width-length ratio can be seen frequently in diastema closure especially in direct technique and affect the proportion, size, and shape of a single tooth appearance and consequently affect the overall esthetic outcome of the final restoration. There have been different reports regarding the length of the maxillary central incisors in the literature. In previously published literature, it has been reported that the length of the maxillary central incisors measured from the gingival margin to the incisal edge should be approximately 10.5–11.0 mm for an esthetic appearance (Fig. 8.6) [5–7]. In another report, it has been stated that the average length of the maxillary central should be 10 mm, with the maximum and minimum lengths being 12 and 8 mm, respectively [8]. Another article reported that the average length of the unworn maxillary central incisors should be 12 mm ranging from 11 to 13 mm [7]. Magne et al. [9] have also reported that the average length of maxillary unworn central incisors measured from the cementoenamel junction to the incisal edge is slightly over 11 mm. For an esthetically pleasant smile, the length of the maxillary central incisors should be between 10.5 and 12 mm, with the average being 11 mm, a good starting point in the esthetic zone according to these authors [9]. In addition, for a natural and perfect appearance, ideal length of the lateral incisors should be 1 mm to 2.5 mm shorter than that of maxillary central incisors (Fig. 8.7) [10, 11]. Maxillary canines should also be slightly shorter than the central incisors ranging between 0.5 mm and 1 mm [10, 11]. The width of the ideal maxillary central incisors should be approximately 8–8.5 mm (Fig. 8.6) for accepted dimensions to create naturally esthetic form [5, 6]. The clinician should always bear in mind that maxillary central incisors are approximately 2–3 mm wider than the lateral incisors and 1–1.5 mm wider than the canines in the esthetic zone (Fig. 8.8) [12]. In addition, maxillary canines should be 1–1.5 mm wider than the laterals, and maxillary central incisors and canines should be positioned 1–1.5 mm incisally than the lateral incisors [12]. Maxillary lateral incisors and canines are also essential clinical evaluation parameters in smile analysis as they play an important role in a pleasing smile. In general, maxillary lateral incisors seem asymmetric in the arch and influence the gender characterization [2, 13]. Maxillary canines are also critical teeth since they are located at the corner of the dental arch. Only the mesial half of these teeth are visible from the frontal aspect when the patient smiles; they can support the upper lips, and position, size, and the shape of these teeth greatly affect the buccal corridor characteristics [2, 13]. In addition, canines and central incisors present gender-specific anatomical differences where feminity is characterized by roundness and smoothness, leading to an oval tooth form with round edges. On the other hand, masculinity is determined by a square shape [2, 13]. The length of the maxillary central incisor shows individual variability depending on the incisal display [8], and patients can have a pleasant smile despite the disproportionate teeth [13]. It has been previously stated that 2 mm tooth size discrepancies in the esthetic zone should be considered as a clinically significant threshold [3, 14]. If the tooth size discrepancy is less than 2 mm, the diastema can be successfully treated with orthodontic treatment [3]. If the tooth size discrepancy exceeds 2 mm, which is confirmed by the tooth size analysis, then a multidisciplinary treatment approach should be considered to enhance the size of the anterior teeth and close the space for an esthetically pleasant outcome [3]. If necessary, the clinician canprepare a diagnostic wax setup (please see Fig. 4.3a, b) for subsequent multidisciplinary evaluation and reconsider the treatment plan [3].
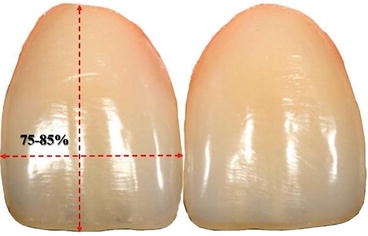
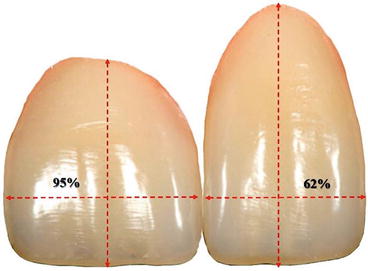



Fig. 8.4
To create an esthetically pleasing and natural final outcome, width to length tooth ratio for maxillary central incisor should be 80 % within the acceptable esthetic range of 75–85 %
Fig. 8.5
Changes in width-length ratio can be seen frequently in diastema closure, and increasing or decreasing these proportions would produce square or rectangular form for a single tooth and would create an unaesthetic appearance
Fig. 8.6
Length of the maxillary central incisors measured from the gingival margin to the incisal edge should be approximately 10.5 to 11.0 mm, and ideal mesiodistal width should be between 8 and 8.5 mm for an esthetic appearance
Fig. 8.7
For a natural and perfect appearance, length of the lateral incisors should be 1 mm to 2.5 mm shorter than that of maxillary central incisors
Fig. 8.8
In the esthetic zone, maxillary central incisor should be approximately 2–3 mm wider than the lateral incisors and 1–1.5 mm wider than the canines
8.2 Dental Model Analysis
According to Andrews, “six keys of the occlusion” are the prerequisites of a normal occlusal relationship [15]. These parameters include molar interarch relationship, mesiodistal crown angulation, labiolingual crown inclination, rotation, tight proximal contacts, and occlusal plane. The inability to achieve proximal contact between all teeth in an arch while maintaining ideal molar intercuspation may indicate a tooth size-arch size discrepancy or a size discrepancy between the maxillary and mandibular teeth. There are several methods of determining the cause of this discrepancy. In this chapter, the most commonly used space and tooth size analysis will be explained. For this purpose, digital models and a software program are most accurate, though standard dental models and a caliper are sufficient.
8.2.1 Space Analysis
Space analysis (Hays Nance analysis) reveals the relationship between tooth size and dental arch length for proper alignment of the teeth in the absence of irregularities or diastemas. This is a basic mathematical equation comparing the required and available space [16]. In each arch, the mesiodistal widths of each tooth mesial to the first permanent molar are summed to determine the “space required” (Fig. 8.9a). To determine the “space available”, the actual arch length is measured using a soft wire shaped to fit the individual arch form and placed on the occlusal surfaces of the teeth, extending from mesial contact point of the right first permanent molar to the mesial contact point of the left first permanent molar (Fig. 8.9b). The difference between the space available and the space required describes the space relationship. A negative value indicates space deficiency leading to crowding, whereas a positive value indicates excess space, which manifests as diastemata. As an alternative to the manual method, software programs can be used (Fig. 8.10).
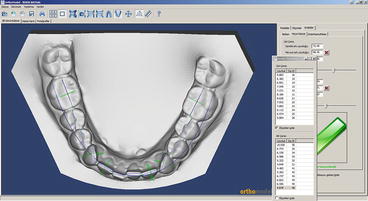
Fig. 8.9
(a) Measurement of mesiodistal tooth widths and (b) measurement of actual arch length. The difference of space available and space required is 4 mm, indicating the amount of diastema
Fig. 8.10
Digital Hays Nance analysis with software program
In diastema cases, Hays Nance analysis calculates the amount of space which should be managed by restorations, orthodontics, or combination of both.
8.2.2 Tooth Size Analysis (Bolton Analysis)
The widths of the maxillary and mandibular teeth must be proportional in order to obtain proper dental interdigitation and arch coordination. However, disproportionate tooth size is quite common [17]. There is a direct relationship between the magnitude of tooth size discrepancies and the presence of occlusal irregularities [18]. Furthermore, a significant crown size difference between upper and lower teeth may prevent achieving a satisfactory occlusion. Excess tooth material in the mandibular arch, for example, may lead to maxillary spacing or mandibular crowding with a Class I molar relationship, or reduced overjet and a Class III molar relationship in properly aligned dental arches without spacing.
Size and shape anomalies of the teeth are most prevalent in upper lateral incisors and upper and lower second premolars [19]. Diminutive maxillary lateral incisors can be easily detected by visually comparing their mesiodistal width with that of the mandibular lateral incisors. In general, a smaller width of the maxillary lateral incisors indicates a discrepancy. When the discrepancy involves several teeth, this process becomes complicated. For a group of teeth (either all anterior teeth or all permanent teeth except second and third molars), Bolton analysis determines the ratio of the mesiodistal widths of the maxillary teeth versus mandibular teeth [20]. First, mesiodistal widths of the permanent teeth are measured, then summed for calculation of the overall ratio using the following formula: overall ratio = (sum of mesiodistal widths of the 12 mandibular teeth)/(sum of mesiodistal widths of the 12 maxillaryteeth) × 100 (Fig. 8.11). If this ratio is greater than 91.3 %, there is excess of mandibular tooth material. If the ratio is smaller than 91.3 %, the excess is in maxilla. The anterior ratio is also calculated using mesiodistal widths of the maxillary and mandibular incisors and canines by the same formula to reveal any discrepancy in the anterior region. If the ratio is greater than 77.2 %, the mandibular anterior teeth are relatively wide compared to the maxillary anterior teeth. If the ratio is smaller than 77.2 %, the maxillary anterior teeth are relatively wide. After calculating the Bolton ratio, a standard table is used to determine the ideal size of this group of teeth based on the assumption that the smaller tooth widths are correct (Tables 8.1 and 8.2). The amount of excess tooth size is then calculated as the difference between actual size and correct size. When using the Bolton analysis to define intermaxillary tooth size discrepancies, the clinician should consider that Bolton’s original data is not applicable to every population [19, 21]. Therefore, population specific norms should be used if available.



Fig. 8.11
Measurement of the mesiodistal widths of the related teeth for Bolton analysis
Table 8.1
Maxillary and mandibular tooth size relationships for 12 teeth
|
Overall ratio
|
|||||
|---|---|---|---|---|---|
|
Max 12
|
Mand 12
|
Max 12
|
Mand 12
|
Max 12
|
Mand 12
|
|
85
|
77.6
|
94
|
85.8
|
103
|
94.0
|
|
86
|
78.5
|
95
|
86.7
|
104
|
95.0
|
|
87
|
79.4
|
96
|
87.6
|
105
|
95.9
|
|
88
|
80.3
|
97
|
88.6
|
106
|
96.8
|
|
89
|
81.3
|
98
|
89.5
|
107
|
97.8
|
|
90
|
82.1
|
99
|
90.4
|
108
|
98.6
|
|
91
|
83.1
|
100
|
91.3
|
109
|
99.5
|
|
92
|
84.0
|
101
|
92.2
|
110
|
100.4
|
|
93
|
84.9
|
102
|
93.1
|
||
Table 8.2
Maxillary and mandibular tooth size relationships for six anterior teeth
|
Anterior ratio
|
|||||
|---|---|---|---|---|---|
|
Max 6
|
Mand 6
|
Max 6
|
Mand 6
|
Max 6
|
Mand 6
|
|
40.0
|
30.9
|
45.5
|
35.1
|
50.5
|
39.0
|
|
40.5
|
31.3
|
46.0
|
35.5
|
51.0
|
39.4
|
|
41.0
|
31.7
|
46.5
|
35.9
|
51.5
|
39.8
|
|
41.5
|
32.0
|
47.0
|
36.3
|
52.0
|
40.1
|
|
42.0
|
32.4
|
47.5
|
36.7
|
||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


