Chapter 66 Current techniques of adenoidectomy
1 INTRODUCTION
The clinical significance of adenoid hypertrophy was not truly appreciated until the mid-19th century. This was due to their relatively inaccessible location given the technology available at that time. Once discovered, various techniques for the removal of the adenoids were developed. Some of these basic techniques have remained with us since that time.
3.1 CURETTE ADENOIDECTOMY
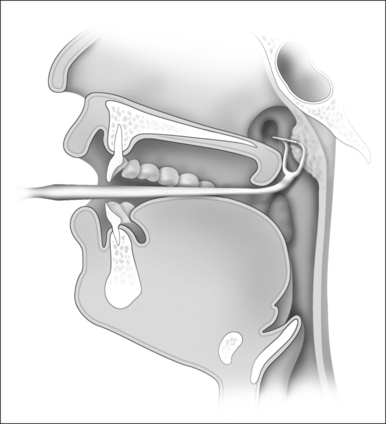
The use of a curette to remove the adenoids dates back to some of the earliest attempts at this procedure and remains an incredibly popular technique worldwide. The original design of Jacob Gottenstein has been modified and many different lengths, widths and curvatures are available. The basic principle is that of a sharp horizontal knife-edge that is designed to cut through the base of the adenoid bed. The instrument is designed to follow the natural curvature of the nasopharyngeal skull base (Fig. 66.1).
3.2 ABLATION ADENOIDECTOMY
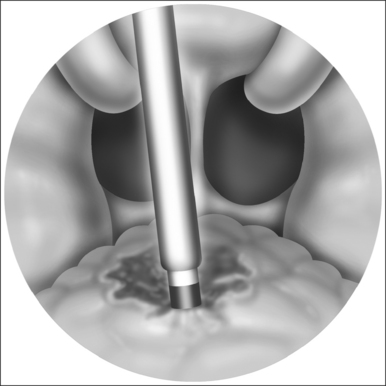
The widespread use of the suction monopolar cautery unit to achieve hemostasis after adenoidectomy naturally led to its use as a primary means of reducing adenoid tissue. With the patient in the Rose position, as described above, the adenoid pad is viewed with a mirror. The monopolar cautery unit, generally set at 30–40 watts, can then be shaped to fit the patient’s unique anatomy. Starting at the choana and working inferiorly, the adenoids are sequentially ablated using the cautery unit (Fig. 66.2). As the tissue fluid is vaporized there is dramatic reduction in the size of the adenoid tissue. Care is taken to avoid inadvertent cautery of non-adenoidal tissue. Bleeding tends to be minimal using this technique and can be controlled with any of the methods described above.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


