Chapter 59 Current techniques for the treatment of velopharyngeal insufficiency
1 INTRODUCTION
Velopharyngeal insufficiency (VPI) is a significant speech disorder. This is usually identified and addressed in childhood, but may be seen as a consequence of central nervous system disease or injury, peripheral nerve injury or palate resection with cancer ablation in the adult. VPIcan be a result of inappropriate articulation and hence, in these cases, remediable by aggressive speech therapy. All too often the treatment will need to be surgical. In this chapter, the surgical treatment will be addressed. Prosthetic management can be quite useful as well and will be addressed in the patient selection section, but will not be fully described here.
2 PATIENT SELECTION
If the decision is made that surgery is necessary, endoscopic evaluation of the velopharynx during speech is needed to decide the type and extent of surgery needed.
3 COMMON CONSIDERATIONS FOR THESEPROCEDURES
The surgery is performed under general anesthesia. Usually the use of an oral RAE tube will allow less interference with the field. The Dingmann mouth gag is usually used. It has the advantage of self-retaining lateral retractors and springs to allow suture retention. Other mouth gags used in tonsil surgery can be employed as well. Craig Senders suggested that releasing the pressure on the tongue during the surgery allowed improved blood flow and likely decreased pain.1
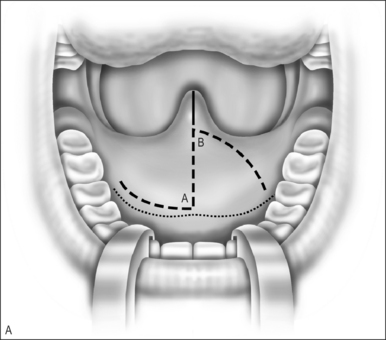
4 FURLOW DOUBLE OPPOSING Z-PLASTY
A Z-plasty lengthens a scar. In VPI the problem often includes a short palate. The double Z-plasty lengthens the palate. The initial ‘Z’ can be made in either direction but the right-handed surgeon seems to do better as pictured (Fig. 59.1A). The posteriorly based flaps are always the myomucosal flaps. The anteriorly based flaps are mucosa only. Kathy Sie suggests rounding the tips of the flaps to improve the vascular supply.2 The incision is carried through the oral cavity mucosa. As the incision is madein the left hemipalate, care must be taken to maintain a small amount of mucosa behind the posterior edge of the hard palate so that suturing is easier. Careful dissection through the levator and tensor veli palatini tendon brings one to the nasal mucosal layer. The plane is usually well defined. Meticulous blunt and sharp dissection separates the undersurface of the muscle bundle from the nasal mucosa.

< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


