To correct an Angle Class II malocclusion or to create spaces in the maxillary arch by nonextraction treatment, distal movement of the maxillary molars is required. Various modalities for distalizing the buccal segment have been reported. Conventional extraoral appliances can be used to obtain maximum anchorage. However, many patients reject headgear wear because of social and esthetic concerns, and the success of this treatment depends on patient compliance. Intraoral appliances, such as repelling magnets, nickel-titanium coils, pendulum appliance, Jones jig appliance, distal jet appliance, and modified Nance appliance, have been introduced to distalize the molars with little or no patient cooperation. However, intraoral appliances can result in anchorage loss of the anterior teeth and distal tipping of the maxillary molars. In this case report, we introduce a diversified rapid maxillary expansion appliance that was custom designed and fabricated for the treatment of a growing girl with a skeletal Class II malocclusion and severe crowding from a totally lingually positioned lateral incisor. The appliance concomitantly expanded the maxilla transversely and retracted the buccal segment sagittally, distalizing the maxillary molars to reach a Class I relationship and creating the spaces to displace the malpositioned lateral incisor. The uniqueness of this special diversified rapid maxillary expansion appliance was highlighted by a series of reconstructions and modifications at different stages of the treatment to reinforce the anchorage.
Highlights
- •
The patient presented with skeletal Class II base with severe crowding highlighted by a palatally malpositioned upper right lateral incisor.
- •
A specially designed diversified RME (DRME) created space for displacement of the malpositioned upper right lateral incisor.
- •
A series of modifications to DRME secured the anchorage that otherwise might have been lost during the molar distalization.
To correct an Angle Class II malocclusion or to create spaces in the maxillary arch by nonextraction treatment, distalization of the maxillary molars is an alternative treatment approach. Various modalities in distalizing the buccal segment have been reported. Conventional extraoral appliances can be used to obtain maximum anchorage. However, many patients reject headgear wear because of social and esthetic concerns, and the success of this treatment depends on patient compliance. Beginning in the 1980s, intraoral appliances, such as repelling magnets, nickel-titanium coils, the pendulum appliance, the Jones jig appliance, the distal jet appliance, and the modified Nance appliance, have been introduced to distalize molars with little or no patient cooperation. However, intraoral appliances can result in anchorage loss of the anterior teeth and distal tipping of the maxillary molars.
In this case report, we introduce a diversified rapid maxillary expander appliance (DRME) that was custom designed and fabricated for the treatment of a girl with a skeletal Class II malocclusion and severe crowding from a totally lingually positioned lateral incisor. The appliance concomitantly expanded the maxilla transversely and retruded the buccal segment sagittally, distalizing the maxillary molars to reach a Class I relationship and creating the spaces to align the remaining maxillary dentition. The uniqueness of this special DRME was highlighted by a series of reconstructions and modifications at different stages of the therapy to reinforce the anchorage.
Diagnosis and etiology
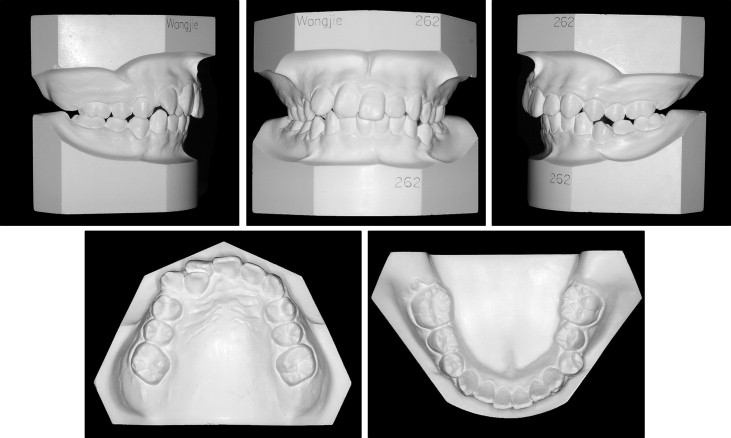
The patient was an 11-year-old Chinese girl with a chief complaint of crooked teeth. The initial clinical examination showed a slightly retrusive mandible with an obtuse nasolabial angle and an increased labiomental fold ( Fig 1 ).

The intraoral examination and study casts exhibited half-step Class II molar relationships on both sides. The maxillary right lateral incisor was completely palatally positioned ( Fig 2 ). The maxillary midline was 4.0 mm off to the right of the facial midline, and the mandibular midline was symmetrically correct. Crowding in the maxilla was severe as a result of an ectopically placed right lateral incisor, whereas crowding in the mandible was mild. The maxilla was constricted, and a crossbite relationship was also noted in the left premolar area. Study cast analysis showed an overbite of 3.0 mm and an overjet of 2.5 mm.
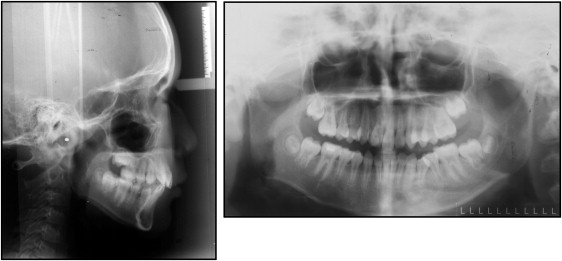
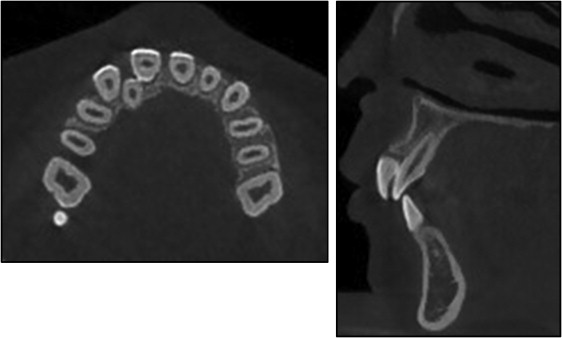
The lateral cephalometric analysis showed a Class II skeletal base (ANB, 5.7°) with a protrusive maxilla (SNA, 86.5°), and an average mandibular plane angle (FMA, 32.8°) ( Fig 3 , Table ). The U1-SN angle of 103.7° indicated a retroclined tendency of the maxillary incisors that might have caused an obtuse nasolabial angle. An inspection of skeletal maturation by the cervical vertebrae suggested considerable growth potential. The panoramic radiograph showed that both maxillary second molars were under development, and the tooth buds of the maxillary third molars did not exist. Furthermore, no pathologic lesions, unusual root formations, or deformities of the maxillary right central or lateral incisors were identified with cone-beam computed tomography ( Fig 4 ).
| Norm | Pretreatment | Posttreatment | Change | |
|---|---|---|---|---|
| SNA (°) | 82.0 ± 3.5 | 86.5 | 84.3 | −2.2 |
| SNB (°) | 77.7 ± 3.2 | 80.8 | 81.5 | 0.7 |
| SN-MP (°) | 32.9 ± 5.2 | 31.7 | 32.7 | 1.0 |
| FMA (°) | 29.2 ± 4.5 | 32.8 | 29.8 | −3.0 |
| ANB (°) | 4.0 ± 1.8 | 5.7 | 2.8 | −2.9 |
| U1-NA (mm) | 4.3 ± 2.7 | 2.6 | 6.3 | 3.7 |
| U1-SN (°) | 103.4 ± 5.5 | 103.7 | 107.3 | 3.6 |
| L1-NB (mm) | 4.0 ± 1.8 | 5.3 | 8.0 | 2.7 |
| IMPA (°) | 95.0 ± 7.0 | 94.1 | 101.3 | 7.2 |
| Lower lip to E-plane (mm) | 2.0 ± 2.0 | 0.4 | 1.1 | 0.7 |
| Upper lip to E-plane (mm) | 1.3 ± 2.0 | 0.4 | −0.2 | −0.6 |
Treatment objectives
The treatment objectives for this patient were to (1) relieve crowding by bringing the palatally positioned lateral incisor into alignment, (2) correct the skeletal Class II, (3) restore a satisfactory occlusion with Class I molar and canine relationships, (4) correct the shifted midline, (5) create ideal overbite and overjet, and (6) improve the facial esthetics.
Treatment objectives
The treatment objectives for this patient were to (1) relieve crowding by bringing the palatally positioned lateral incisor into alignment, (2) correct the skeletal Class II, (3) restore a satisfactory occlusion with Class I molar and canine relationships, (4) correct the shifted midline, (5) create ideal overbite and overjet, and (6) improve the facial esthetics.
Treatment alternatives
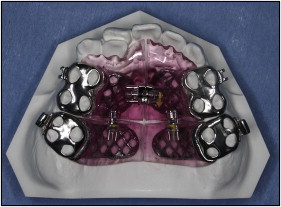
This preteen patient had adequate growth potential, with an acceptable profile but with a retroclined maxillary anterior dentition. A maxillary lateral incisor was palatally positioned, but there were no signs of defects in the overlapping areas between the adjacent dentition ( Fig 4 ). Furthermore, the maxillary second molars were not erupted, indicating that the timing for molar distalization might be an acceptable treatment modality. A nonextraction treatment plan was therefore proposed. The first step was orthopedic treatment with a specially designed DRME ( Fig 5 ). This appliance was designed to expand the maxillary arch and distalize the maxillary molars simultaneously to create spaces for crowding relief and restoration of the molar relationship. The second step was orthodontic treatment with fixed appliances to improve the buccal interdigitation and establish a proper incisal relationship. Microimplant anchorage devices (MIAs) could be applied in the maxilla to retract the frontal segment because the frontal anchorage might be partially lost as a result of buccal segmental distalization.
In the maxillary arch, by moving the buccal dentition posteriorly, the maxillary left quadrant was to be distalized for midline correction, and crowding of the right quadrant was to be relieved. In the mandibular arch, mild crowding was to be relieved by expansion with broad archwires, whereas the sagittal position of the anterior teeth would remain to prevent further deepening of the labiomental fold.
Over the whole course of orthopedic treatment, the adaptive modifications to the DRME would remain a constant endeavor to secure the frontal segment anchorage against the buccal distalization and vice versa.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


