This article describes an orthodontic system used to obtain active continuous torque with movement control of both active and reactive units; the system relies on principles of the segmented technique. A cantilever system with .017 x .025-in beta-titanium alloy wire was designed to provide the desirable moment on the active unit. A transpalatal bar or a lingual arch increases the anchorage and neutralizes the side effects on the reactive unit. This technique is an efficient approach for major corrections of buccolingual inclinations of certain teeth.
The objectives of orthodontic treatment include obtaining functional occlusion, good esthetics, and stable results. Ideal buccolingual inclination of the posterior and anterior teeth after active treatment is considered essential. Orthodontists can use a preadjusted appliance and a continuous archwire to move teeth; in this system, the teeth should follow the shape of the arch to reach a position close to ideal. Based on their properties, the wire deflects at sites of misaligned tooth and returns to its initial position after correction of the malpositioned tooth. Sometimes, bends must be included to obtain the desired movement; however, these bends can be transmitted to the anchorage tooth, with undesirable side effects. When a continuous archwire is used to produce active torque to control the axial inclination of teeth, an opposite and undesirable torque reaction is produced over adjacent teeth or segments of the arch from flexion of the archwire, and some side effects are possible. For small tooth movements, this system can work well, but it is less effective for major corrections because of the risk of damage, especially if the adjacent tooth is smaller than the active torque unit. This often happens when torque is needed in the canine area. Several attempts have been made to compensate. Segmented arch mechanics can be used to control tooth movement, reducing many undesirable side effects on adjacent teeth. The advantage of this approach is that it allows the possibility of developing an accurate and predictable system of force.
According to orthodontic biomechanics, if the line of force does not pass through the center of resistance, some rotation will occur. This tendency to rotate is measured as a moment (M), which is equal to force (F) magnitude multiplied by the perpendicular distance (D) between the line of force to the center of resistance (M = F × D). The movement type of a tooth is determined by the ratio between the magnitude of moment and the force applied at the bracket (M:F ratio). Varying the M:F ratio produces various centers of rotation, which determine different types of tooth movement. When the M:F ratio is 12:1 or more, the center of rotation will be at the incisal edge, resulting in tooth movement with minor crown movement.
In this article, we describe an appliance designed to obtain active continuous torque and control tooth movement with a known M:F ratio. The aim is an optimal biologic response by delivering a constant force at an optimal magnitude.
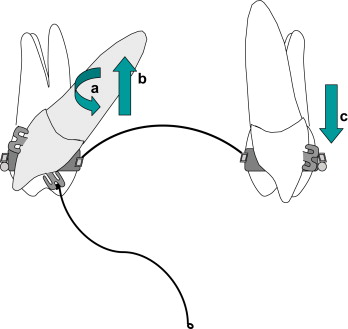
This orthodontic system uses the principles of the segmented-arch technique. The system acts as a cantilever; at one end, the spring is placed into a slot of the bracket bonded to the palatal or lingual surface of the tooth, and at the other end of the spring, one helicoid is tied into the transpalatal bar or the lingual arch near the lingual tube, with a 0.025-mm ligature wire as 1 point of contact ( Fig 1 ). This cantilever is usually made of 0.017 × 0.025-in beta-titanium alloy wire. To provide anchorage reinforcement, either a passive transpalatal bar or a lingual arch is used with a heavy buccal archwire, such as 0.019 × 0.025-in stainless steel if the slot is 0.022 in, or 0.017 × 0.025 in for an 0.018-in slot. The bracket bonded to the palatal surface can be any one whose base adapts well to the contour of the bonded surface, and in which slot the wire is fully engaged.
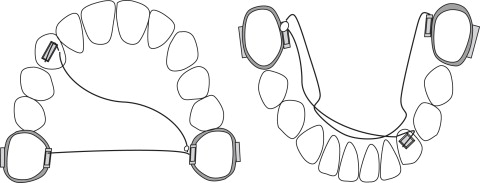
The cantilever characterizes a statically determinate system with the forces and the moments readily measured; this makes the release of light and constant forces possible without changes of the system of forces during deactivation or movement of the active element. This system gives a desirable combination of moments and forces on the activated side (where the wire is placed in the bracket), whereas on the reactive side only force is delivered ( Fig 2 ). However, the effect on the reactive side is seldom considered a problem in clinical experience, because of the stabilizing effect of either the transpalatal bar, or both the lingual arch and the buccal archwire, and because of the low load-to-deflection ratio; because the cantilever is long and fabricated with beta-titanium alloy wire, this ratio is low, providing a biologic movement with a high moment and a small vertical force. The force transmitted to the active unit is, in some cases, undesirable; the heavy buccal archwire can minimize or nullify unwanted reactive effects ( Fig 3 ).