Inroduction
Our objective was to assess tooth wear, arch dimensions, tooth sizes, and dental crowding in 4 remote indigenous villages on the Xingu River in Brazil. These populations have similar patterns of dietary habits and practice exclusive breast-feeding, whereas studies in human genetics show large intertribal genetic distances and low intratribal variations.
Methods
Dental casts of 107 subjects in the permanent dentition were evaluated. Tooth wear, arch dimensions, mesiodistal tooth widths, and the irregularity index of the incisors were obtained and compared using analysis of variance or the Kruskal-Wallis test ( P <0.05).
Results
Tooth wear and tooth size in the mandible were similar among villages. Three groups were discriminated. The first group included the Xicrin-Kayapó and Arara-Laranjal villages, since no significant difference was found between them. Larger tooth sizes and arch dimensions ( P <0.001) were found in both jaws in the Assurini village compared with the Xicrin-Kayapó and Arara-Laranjal villages; this resulted in similar dental crowding index values in these groups. The Arara-Iriri village, where a high coefficient of inbreeding had been reported, showed intermediate arch dimensions, with the mesiodistal tooth widths similar to those in the Xicrin-Kayapó and Arara-Laranjal villages. This scenario resulted in a group with the lowest irregularity index, close to 0.
Conclusions
These Amazonian indigenous villagers, who have been genetically studied previously, showed large intergroup genetic variations and similar patterns of tooth wear. Thus, we suggest from the findings in this study that the etiology of dental crowding among the inhabitants of the Xingu River area is predominantly associated with variations in the dimensions of dental arches, related to genetic influences.
Highlights
- •
Roles of genetics and environment in tooth and arch dimensions have not been determined.
- •
Examining remote populations is an opportunity to investigate this issue.
- •
Etiology of dental crowding is predominantly associated with genetic variations.
- •
Genetics contribute greatly to the dimensions of the dental arches.
Dental malocclusions occur because of an abnormal relationship between the dental arches or changes in tooth position from intra-arch alterations. Among these intra-arch alterations, dental crowding is the most frequent, leading to orthodontic treatment for millions of people worldwide.
Scientifically, dental crowding has been called a “disease of civilization.” Studies of human and nonhuman primates have shown that the increased occurrence of this malocclusion should be attributed to the food manufacturing process. Arguably, the increasing availability of soft foods could cause a reduction in masticatory force, an important mechanism for fostering dental arch growth and reducing tooth mass as a result of tooth wear. Moreover, studies of ancient populations, including indigenous Amazonian peoples, have shown dental crowding even with tooth wear.
The influence of tooth size and dental arch dimensions on the emergence of crowding is yet another controversial issue. Although a consensus has been reached regarding the role of dental arch dimensions in crowding, the association between dental crowding and tooth size is inconclusive. One group of studies reported a significant correlation, but other studies have shown slight or insignificant associations.
The roles of genetics and the environment in tooth morphology and dental arch dimensions, as well as the relationship between these variables and dental crowding, are still fraught with controversy. Examining 4 indigenous populations, on which previous reports have indicated low intratribal genetic variations combined with large intertribal variations and preserved dietary habits, provides an interesting opportunity to investigate factors related to the development of irregularities in tooth position, which might survive camouflaged in modern populations.
Material and methods
The participants provided written or verbal informed consent in their native languages to be included in this study. Verbal consent was recorded for adults who could not sign. Informed consent from guardians was also obtained for the minors and children enrolled in the study. The Brazilian National Research Ethics Committee approved the informed consent and the study protocol (25000.066559/2011).
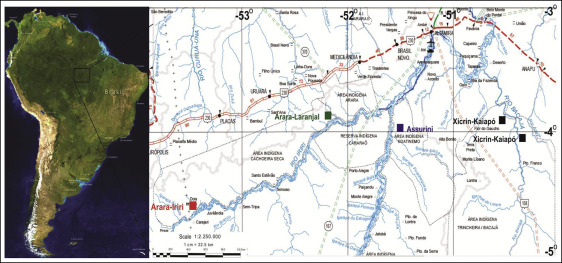
This study was done among indigenous peoples from villages on the Xingu River, a tributary of the Amazon River ( Fig 1 ). All inhabitants of the villages were examined clinically. Thereafter, those who were in the deciduous or mixed dentition and older than 50 years were excluded, so that only subjects in the permanent dentition with all permanent teeth except the third molars were included in the study ( Table I ).
| Sex | Assurini (n = 22) | Xicrin-Kaiapó (n = 30) | Arara-Iriri (n = 20) | Arara-Laranjal (n = 35) | ||||
|---|---|---|---|---|---|---|---|---|
| n (%) | Age (y) | n (%) | Age (y) | n (%) | Age (y) | n (%) | Age (y) | |
| Male | 12 (54.5) | 17.9 | 16 (53.3) | 18.3 | 10 (50) | 17.1 | 19 (54.3) | 17 |
| Female | 10 (45.5) | 17 | 14 (46.7) | 21.1 | 10 (50) | 15.8 | 16 (45.7) | 15.2 |
| Total | 22 (100) | 17.7 | 30 (100) | 18.9 | 20 (100) | 16.6 | 35 (100) | 15.9 |
Measurements were made on the dental casts of 107 subjects for biometric examinations of tooth sizes and dental arch dimensions. They included 22 people from the Assurini, 30 from the Xicrin-Kayapó, 20 from the Arara-Iriri, and 35 from the Arara-Laranjal ethnic groups. The numbers of subjects by sex were similar among the groups ( Table I ).
The mesiodistal diameters of permanent teeth, intermolar and intercanine widths, diagonal lengths of the arches, and the irregularity index of the anterior teeth were obtained by 1 examiner (H.G.A.S.) with a 150-mm digital caliper with 0.01-mm resolution (CE 03.040487ECC; TÜV Rheinland, Cologne, Germany). After 30 days, the measurements were duplicated; a difference greater than 1 mm required a third measurement, which replaced the most discrepant value.
Statistical analysis
The method error for the measurements was found by comparing 2 measurements taken at different times on 15 dental casts. Dahlberg’s formula was applied to determine random errors, and the paired Student t test was used to evaluate systematic errors.
With the limited sample because of the size of the populations studied, a compromised sample size was calculated, assuming a power of 80% and a standard deviation of 2 mm for Little’s irregularity index, according to the data in a previous report. Thus, a sample of 16 subjects per group would have 80% power to read a 2-mm difference, and a sample of 27 subjects per group would have the same power to read a difference of 1.5 mm.
For the analysis of dental wear, the modified index by Mockers et al was used to examine the wear on the occlusal surfaces of the first and second premolars, canines, and lateral and central incisors in both arches. The following scores were recorded for each tooth: 0, no wear; stage 1, wear of the enamel only; stage 2, wear of the dentin, in which the occlusal surface has more enamel than dentin; stage 3, wear of the dentin, in which the occlusal surface has more dentin than enamel; and stage 4, advanced wear, either close to or with exposure of the pulp chamber. For each subject, an arithmetic mean for tooth wear was obtained as described by Normando et al.
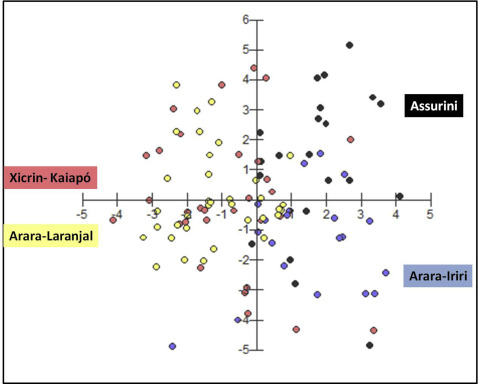
Data normality was examined with the Shapiro-Wilk test. When the data showed normality, analysis of variance (ANOVA) followed by the Tukey test was used. In case of abnormality or heteroscedasticity, ANOVA was replaced by the Kruskal-Wallis test, followed by the Dunn test. Discriminant analysis was used to draw a graph.
For all statistical analyses, including sample size calculation, the βioEstat software (version 5.3; Mamirauá Institute, Belém, Pará, Brazil) was used.
Results
The random errors ranged between 0.61 and 0.19 mm ( P >0.05) ( Table II ).
| Variable (mm) | Random error | Male and female | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Xicrin-Kaiapó (n = 30) | Arara-Laranjal (n = 35) | Arara-Iriri (n = 20) | Assurini (n = 22) | P value | ||||||
| Dalhberg | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Tooth wear | 0.13 (NS) | 0.41 | 0.27 | 0.56 | 0.45 | 0.7 | 0.62 | 0.67 | 0.44 | 0.08 (NS) b |
| Maxillary arch | ||||||||||
| Intermolar | 0.28 (NS) | 53.54 b | 2.56 | 53.34 b | 1.89 | 53.67 b | 3.06 | 56.2 a | 2.7 | 0.0005 |
| Intercanine | 0.19 (NS) | 36.04 b | 1.62 | 36.1 b | 1.71 | 37.73 a | 1.75 | 38.78 a | 1.83 | <0.0001 |
| Arch length | 0.46 (NS) | 65.71 c | 3.94 | 64.23 c | 2.6 | 67.49 b | 4.56 | 70.18 a | 4.6 | <0.0001 ∗ |
| Tooth size ∑5-5 | 0.61 (NS) | 75.69 b | 3.27 | 75.95 b | 2.68 | 76.27 b | 2.66 | 78.78 a | 4.69 | 0.0127 ∗ |
| Little’s index | 0.32 (NS) | 4.23 a | 4.05 | 2.57 a | 3.12 | 0.79 b | 1.29 | 2.93 a | 2.32 | 0.0008 ∗ |
| Mandibular arch | ||||||||||
| Intermolar | 0.24 (NS) | 45.23 b | 3.18 | 45.32 b | 1.82 | 45.26 b | 1.76 | 47.65 a | 2.24 | 0.0027 ∗ |
| Intercanine | 0.3 (NS) | 27.55 b | 2.51 | 27.56 b | 1.6 | 28.14 ab | 1.22 | 29.08 a | 2.01 | 0.0392 ∗ |
| Arch length | 0.38 (NS) | 56.51 bc | 3.89 | 55.76 c | 2.56 | 58.26 ab | 2.84 | 59.97 a | 3.21 | <0.0001 |
| Tooth size ∑5-5 | 0.35 (NS) | 66.17 a | 3.34 | 65.93 a | 2.58 | 65.4 a | 2.58 | 67.78 a | 3.99 | 0.068 (NS) ∗ |
| Little’s index | 0.44 (NS) | 3.74 a | 3.49 | 3.54 a | 2.67 | 1.28 b | 1.87 | 4.48 a | 2.9 | 0.0016 ∗ |
Tooth wear when comparing the 4 groups showed no difference ( P = 0.08), with mean values between 0.69 and 0.41 ( Table II ).
The analysis of tooth size showed that the differences between all indigenous groups were not significant in the mandibular arch ( Table II ). However, greater maxillary tooth sizes were found in the Assurini group compared with the other ethnic groups ( Table II ). The sum of mesiodistal tooth diameters was about 2.5 to 3.1 mm greater in the Assurini group compared with the other indigenous groups ( P <0.01). No significant difference in tooth size in the maxilla was observed between the Arara (Laranjal and Iriri) and the Xicrin-Kayapó subjects.
Regarding the maxillary arch dimensions, the subjects from the Xicrin-Kayapó and Arara-Laranjal villages generally exhibited similar dimensions, but these were smaller than those in the Assurini group ( Table II ). Compared with the Arara-Iriri, the Assurini group tended to have larger dimensions in the maxilla. The Arara-Iriri subjects showed larger arch dimensions compared with the Arara-Laranjal, who were of the same ethnicity, and with the Xicrin-Kayapó subjects. The difference was statistically significant for intercanine width (1.63 mm; P <0.01) and arch length (3.23 mm; P <0.01) compared with the Arara-Laranjal, and for intercanine width (1.69 mm; P <0.01) and arch length (1.78 mm; P <0.01) compared with the Xicrin-Kayapó. No differences in intermolar width were observed among these 3 groups.
An analysis of the mandibular arch dimensions confirmed the trend observed in the maxillary arch. The dimensions were significantly greater in the Assurini than in the other groups. Compared with the Arara-Iriri, only intermolar width was statistically greater, around 2.4 mm. The Xicrin-Kayapó and Arara groups showed no significant differences in mandibular dimensions. However, between the 2 Arara groups, the length of the mandibular arch was 2.5 mm shorter in the Arara-Laranjal group ( P <0.01).
The contrast between tooth size and dental arch dimensions allows an assessment of bone-tooth discrepancies. Although the Assurini had larger teeth, mainly the maxillary ones, than did the subjects from the other indigenous villages, they also had larger dental arches. The combination of larger teeth and arches did not result in any significant differences in dental crowding between the Assurini group compared with the Xicrin-Kayapó and Arara-Laranjal villages, with the latter having significantly smaller arches and teeth than the Assurini.
On the other hand, the Arara-Iriri group exhibited discriminant behavior in tooth irregularity compared with the other indigenous groups ( Fig 2 ). This group had teeth with mesiodistal diameters similar to those of the Xicrin-Kayapó and Arara-Laranjal groups, although their arch dimensions were significantly greater than in these other groups. Thus, the Arara-Iriri had the lowest tooth irregularity index values for both maxillary (0.79 mm) and mandibular (1.28 mm) arches. These values were significantly lower than those in the other groups ( P <0.001).