Introduction
With the advent of cone-beam computed tomography (CBCT) scans, there has been a transition toward these scans’ replacing traditional radiographs for orthodontic diagnosis and treatment planning. Children represent a significant proportion of orthodontic patients. Similar CBCT exposure settings are predicted to result in higher equivalent doses to the head and neck organs in children than in adults. The purpose of this study was to measure the difference in equivalent organ doses from different scanners under similar settings in children compared with adults.
Methods
Two phantom heads were used, representing a 33-year-old woman and a 5-year-old boy. Optically stimulated dosimeters were placed at 8 key head and neck organs, and equivalent doses to these organs were calculated after scanning. The manufacturers’ predefined exposure settings were used.
Results
One scanner had a pediatric preset option; the other did not. Scanning the child’s phantom head with the adult settings resulted in significantly higher equivalent radiation doses to children compared with adults, ranging from a 117% average ratio of equivalent dose to 341%. Readings at the cervical spine level were decreased significantly, down to 30% of the adult equivalent dose. When the pediatric preset was used for the scans, there was a decrease in the ratio of equivalent dose to the child mandible and thyroid.
Conclusions
CBCT scans with adult settings on both phantom heads resulted in higher radiation doses to the head and neck organs in the child compared with the adult. In practice, this might result in excessive radiation to children scanned with default adult settings. Collimation should be used when possible to reduce the radiation dose to the patient. While CBCT scans offer a valuable tool, use of CBCT scans should be justified on a specific case-by-case basis.
The development of cone-beam computed tomography (CBCT) has introduced a transition toward these scans’ replacing traditional radiographs taken for orthodontic diagnosis and treatment planning. Since children are a significant proportion of orthodontic patients, the use of the same CBCT exposure settings for children and adults is predicted to result in higher equivalent doses to the head and neck organs in children than in adults. The CBCT radiation exposure to the surface tissues of adults has been previously measured with adult male phantom heads using thermo-luminescent dosimeters (TLDs). However, to our knowledge, a comparative characterization of the radiation exposure from different CBCT scanners in children and adults is not available.
Once cancer risk from x-ray radiation was confirmed early in the 20th century, the International Commission on Radiological Protection (ICRP) has worked hard to develop guidelines for x-ray exposure and safety protocol. In the 1990s, the ICRP moved toward using the equivalent and effective dose (measured in microsieverts) as a measure of organ dose and biologic risk, instead of the more traditional absorbed dose. The equivalent dose takes into account tissue sensitivity to radiation and provides a more accurate picture of the detrimental effects of radiation to the patient. Although simple periapical x-rays expose patients to the equivalent of a few days’ worth of background radiation and potentially increase cancer risk by less than 1 in 1,000,000, medical computed tomography (CT) scans expose patients to the equivalent of 2 to 3 years of background radiation and potentially increase cancer risk by 1 in 1000 to 1 in 10,000. CBCT scans offer an alternative to medical CT imaging, with comparable quality of bony images but much less radiation, and they are significantly less expensive.
In recent years, more orthodontists have moved toward using CBCT scans for diagnosis, as they offer a “1 scan covers all” type of convenience to practitioners. The rapid adoption of CBCT into practice has outstripped the time needed to conduct well-controlled studies on x-ray radiation from CBCT and to implement or suggest guidelines on CBCT use. Whereas radiation exposure from CBCT has been shown to be less than that from multidetector CT used in medicine, it is still greater relative to conventional dental radiographs.
Radiographic examination should be performed only when indicated by the patient’s dental history, the dentist’s physical examination, or laboratory findings. Justification of radiographic examination in children is especially important since children’s tissues are different in size and position and are under constant growth, replication, and differentiation, making them significantly more susceptible to radiation damage compared with adult tissues. Radiation risk highly depends on age, with risk inversely proportional to age; for the same radiation doses, children less than 10 years of age have about a 3-times higher risk than a 30-year-old adult. In addition, the risk for females is typically higher than that for males.
Previous studies evaluating radiation doses to phantom heads from CBCT scans have used TLDs on adult male phantom heads. In this study, we used optically stimulated luminescent (OSL) dosimeters (NanoDot; Landauer, Glenwood, Ill). This is a newer technology of dosimeters, which we used to characterize CBCT radiation exposure to a woman’s phantom head and a child’s phantom head. The advantages of OSL dosimeters over TLDs include faster readouts and more accurate readings, as the OSL dosimeters are optically stimulated with green light, which is more efficient than the thermally stimulated TLDs. OSL dosimeters also allow for multiple exposures and readouts from 1 dosimeter, have lower depletion over time, and are more sensitive than TLDs.
Few studies have evaluated the differences in radiation dose from CBCT scans to adults compared with children. Data characterizations of the equivalent organ doses from different CBCT scanners under similar controlled settings are limited in the literature. The purpose of this study was to measure the differences in equivalent organ dose from different scanners under similar settings in children compared with adults. We investigated the equivalent doses to the lens of the eye, the thyroid, and several head and neck organs of an anthropomorphic adult female phantom head and an anthropomorphic child male phantom head. The data were obtained from 2 commercially available dental CBCT scanners using several specific exposure settings.
Material and methods
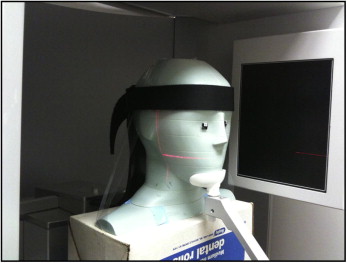
Two phantom heads were used: an adult female anthropomorphic phantom (model 702; Computerized Reference Imaging System, Norfolk, Va) corresponding to an average 33-year-old woman who is 160 cm in height and 55 kg in weight ( Fig 1 ) and a child male anthropomorphic phantom (model 705; Computerized Reference Imaging System) corresponding to an average 5-year-old boy who is 110 cm in height and 19 kg in weight. OSL dosimeters were placed at 8 key head and neck organs in the 2 phantom heads to assess the radiation doses ( Table I ; Fig 2 ). Equivalent doses to the head and neck organs were calculated based on the 2007 recommendations of the ICRP. The i-CAT Platinum CBCT scanner (Imaging Sciences International, Hatfield, Pa) with 5 manufacturer-predefined exposure settings and the Iluma CBCT scanner (IMTEC, Ardmore, Okla) with 4 predefined settings were used in this study. Preset pediatric settings, only available in the Iluma scanner, were used with the child phantom head. For the Iluma, 2 scanning techniques were used: the full-head scan with no collimation and the collimated scan (collimated to the maxillary-mandibular area, excluding the eyes). Both scanning techniques had the same machine parameters of 120 kV(p) and 3.8 mA. For the i-CAT, full-head, maxilla-only, and mandible-only scans were taken, all using the same machine parameters of 120 kV(p) and 5 mA. Table II shows the parameters for each scan. The scans were repeated by the same investigators (L.T.D., G.P., R.P., A.D.G.) 3 times (scout and volumetric acquisitions), and radiation exposure to the OSL dosimeters was read with a MicroStar reader (Landauer, Glenwood, Ill). Specific labeled dosimeters were used for each site. The dosimeters were measured before exposure for a background reading, exposed, and then read again. All dosimeters were read 3 times, and background radiation readings were subtracted from the average readings to give the radiation dose to the dosimeter. Individual readings of absorbed dose for each scan (scout plus volumetric acquisitions) were obtained by dividing the average readings minus the background by 3. Dosimetrical statistical evaluations were calculated using Excel (Microsoft, Redmond, Wash). Averaged radiation readings were then converted to equivalent doses using the tissue-weighting factors of the 2007 ICRP’s recommendations. The calculated child equivalent doses were divided by the adult equivalent dose, giving a percentage ratio of child over adult comparison of the equivalent dose. This study will help to develop a baseline for other CBCT studies to follow.
| Adult (n) | Child (n) | |
|---|---|---|
| Brain | 8 | 3 |
| Cranium | 4 | 3 |
| Eye | 2 | 2 |
| Mandible | 2 | 2 |
| Cervical spin | 1 | 2 |
| Thyroid | 2 | 4 |
| Parotid | 2 | 1 |
| Eye lens | 2 | 2 |

| Type of scan | Resolution (mm) | Exposure time (s) | Kilovoltage (kV[p]) | Current (mA) |
|---|---|---|---|---|
| i-CAT | ||||
| Full head | 0.3 | 8.9 | 120 | 5 |
| Maxilla | 0.2 | 26.9 | 120 | 5 |
| Maxilla | 0.4 | 8.9 | 120 | 5 |
| Mandible | 0.2 | 26.9 | 120 | 5 |
| Mandible | 0.4 | 8.9 | 120 | 5 |
| Iluma | ||||
| Full head | 0.3 | 7.8 | 120 | 3.8 |
| Maxilla-mandible | 0.2 | 40 | 120 | 3.8 |
| Maxilla-mandible | 0.4 | 20 | 120 | 3.8 |
| Maxilla-mandible | 0.2 | 7.8 | 120 | 3.8 |
Results
Readings from the i-CAT, which did not have a pediatric preset option, showed significantly higher equivalent doses to children compared with adults, ranging from a 117% average ratio of equivalent dose increase for a 3-mm full-head scan, to a 173% average increase for the 0.4-mm maxilla scan ( Table III ). The child’s mandible received an equivalent radiation dose 341% higher than the adult dose for the 0.4-mm maxilla scan, the highest increase in relative effective dose. Brain and cranial tissues received equivalent doses of 152% to 295% higher than adults, depending on the resolution of the scan and collimation. Readings at the cervical-spine level, however, were decreased significantly to 30% of the adult equivalent dose. The mandible and the parotid also showed decreases in equivalent doses to children, although not as dramatic as those at the cervical-spine level ( Table III ).
| Full head 0.3 mm (%) | Maxilla 0.2 mm (%) | Maxilla 0.4 mm (%) | Mandible 0.2 mm (%) | Mandible 0.4 mm (%) | |
|---|---|---|---|---|---|
| Brain | 152 | 200 | 214 | 233 | 180 |
| Cranium | 160 | 295 | 279 | 286 | 257 |
| Mandible | 127 | 325 | 341 | 94 | 99 |
| Cervical spine | 30 | 29 | 34 | 34 | 32 |
| Thyroid | 140 | 130 | 143 | 118 | 133 |
| Parotid | 90 | 92 | 101 | 115 | 119 |
| Average child/adult | 117 | 170 | 173 | 145 | 137 |
On the other hand, the Iluma had a pediatric preset that was used for the scans. Increases for average equivalent dose ranged from 158% for the 7.8-second full-head scan to 266% for the 20-second collimated maxilla-mandible scan ( Table IV ). Brain and cranial tissues received an equivalent radiation dose increase of up to 479% in the 7.8-second full-head scan. Preliminary data on the eye dosimeters measured the highest increase at 671% in equivalent dose for the 20-second collimated maxilla-mandible scan. Further findings on the eye and lens dosimeters will be published later. Similar to the i-CAT measurements, the cervical spine showed significant decreases in equivalent radiation, down to 54% to 68% of the adult equivalent dose. The mandible and thyroid also showed decreases in equivalent doses relative to the adult readings, to as low as 75% ( Table IV ).
| Full scan 7.8 s (%) | Collimated maxilla-mandible 40 s (%) | Collimated maxilla-mandible 20 s (%) | Collimated maxilla-mandible 7.8 s (%) | |
|---|---|---|---|---|
| Brain | 212 | 329 | 346 | 413 |
| Cranium | 479 | 373 | 378 | 367 |
| Mandible | 85 | 101 | 102 | 86 |
| Cervical spine | 68 | 61 | 54 | 63 |
| Thyroid | 93 | 75 | 77 | 75 |
| Parotid | 117 | 97 | 103 | 132 |
| Average child/adult | 176 | 173 | 177 | 189 |
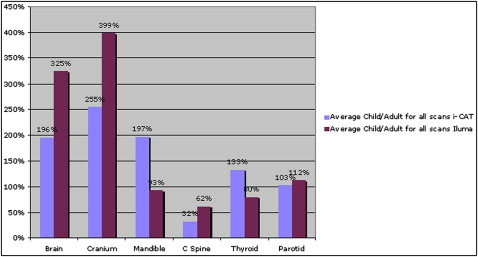
Comparing the equivalent dose percentages between the i-CAT and the Iluma showed that the Iluma’s pediatric settings decreased the radiation to the mandible and thyroid, with similar results at the parotid. However, the i-CAT had significantly lower radiation delivery to the brain, cranium, and cervical spine ( Tables III and IV ; Fig 3 ). Tables V through XIII show the equivalent radiation dose readings for adults and children for each organ from the various scans.
| Adult | Child | Ratio of equivalent dose child/adult (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Organ dose (cGy) | SD | W T (ICRP 103) | Equivalent dose (μSv) | Organ dose (cGy) | SD | W T (ICRP 103) | Equivalent dose (μSv) | ||
| Brain | 0.066 | 0.008 | 0.01 | 6.6 | 0.1 | 0.01 | 0.01 | 10.0 | 152 |
| Cranium | 0.05 | 0.01 | 0.01 | 5.0 | 0.08 | 0.01 | 0.01 | 8.0 | 160 |
| Mandible | 0.079 | 0.008 | 0.01 | 7.9 | 0.1 | 0.02 | 0.01 | 10.0 | 127 |
| Cervical spine | 0.109 | 0.002 | 0.01 | 10.9 | 0.033 | 0.0004 | 0.01 | 3.3 | 30 |
| Thyroid | 0.02142 | 0.00009 | 0.04 | 8.6 | 0.03 | 0.01 | 0.04 | 12.0 | 140 |
| Parotid | 0.11 | 0.02 | 0.01 | 11.0 | 0.0986 | 0.0001 | 0.01 | 9.9 | 90 |
| Average child/adult | 116 | ||||||||
| Adult | Child | Ratio of equivalent dose child/adult (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Organ dose (cGy) | SD | W T (ICRP 103) | Equivalent dose (μSv) | Organ dose (cGy) | SD | W T (ICRP 103) | Equivalent dose (μSv) | ||
| Brain | 0.03 | 0.02 | 0.01 | 3.0 | 0.06 | 0.03 | 0.01 | 6.0 | 200 |
| Cranium | 0.0088 | 0.0009 | 0.01 | 0.9 | 0.026 | 0.001 | 0.01 | 2.6 | 295 |
| Mandible | 0.083 | 0.001 | 0.01 | 8.3 | 0.27 | 0.02 | 0.01 | 27.0 | 325 |
| Cervical spine | 0.1074 | 0.0006 | 0.01 | 10.7 | 0.0315 | 0.0001 | 0.01 | 3.2 | 29 |
| Thyroid | 0.023 | 0.002 | 0.04 | 9.2 | 0.03 | 0.01 | 0.04 | 12.0 | 130 |
| Parotid | 0.3 | 0.02 | 0.01 | 30.0 | 0.277 | 0.004 | 0.01 | 27.7 | 92 |
| Average child/adult | 179 | ||||||||
| Adult | Child | Ratio of equivalent dose child/adult (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Organ dose (cGy) | SD | W T (ICRP 103) | Equivalent dose (μSv) | Organ dose (cGy) | SD | W T (ICRP 103) | Equivalent dose (μSv) | ||
| Brain | 0.014 | 0.009 | 0.01 | 1.4 | 0.03 | 0.01 | 0.01 | 3.0 | 214 |
| Cranium | 0.0043 | 0.0009 | 0.01 | 0.4 | 0.012 | 0.001 | 0.01 | 1.2 | 279 |
| Mandible | 0.0411 | 0.0005 | 0.01 | 4.1 | 0.14 | 0.01 | 0.01 | 14.0 | 341 |
| Cervical spine | 0.0468 | 0.0008 | 0.01 | 4.7 | 0.016 | 0.003 | 0.01 | 1.6 | 34 |
| Thyroid | 0.0112 | 0.0006 | 0.04 | 4.5 | 0.016 | 0.007 | 0.04 | 6.4 | 143 |
| Parotid | 0.146 | 0.009 | 0.01 | 14.6 | 0.1469 | 0.0002 | 0.01 | 14.7 | 101 |
| Average child/adult | 185 | ||||||||
| Adult | Child | Ratio of equivalent dose child/adult (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Organ dose (cGy) | SD | W T (ICRP103) | Equivalent dose (μSv) | Organ dose (cGy) | SD | W T (ICRP103) | Equivalent dose (μSv) | ||
| Brain | 0.009 | 0.006 | 0.01 | 0.9 | 0.021 | 0.009 | 0.01 | 2.1 | 233 |
| Cranium | 0.0028 | 0.0006 | 0.01 | 0.3 | 0.008 | 0.001 | 0.01 | 0.8 | 286 |
| Mandible | 0.28 | 0.02 | 0.01 | 28.0 | 0.262 | 0.006 | 0.01 | 26.2 | 94 |
| Cervical spine | 0.249 | 0.005 | 0.01 | 24.9 | 0.0856 | 0.0002 | 0.01 | 8.6 | 34 |
| Thyroid | 0.0593 | 0.0002 | 0.04 | 23.7 | 0.07 | 0.04 | 0.04 | 28.0 | 118 |
| Parotid | 0.25 | 0.02 | 0.01 | 25.0 | 0.288 | 0.004 | 0.01 | 28.8 | 115 |
| Average child/adult | 147 | ||||||||
| Adult | Child | Ratio of equivalent dose child/adult (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Organ dose (cGy) | SD | W T (ICRP 103) | Equivalent dose (μSv) | Organ dose (cGy) | SD | W T (ICRP 103) | Equivalent dose (μSv) | ||
| Brain | 0.005 | 0.003 | 0.01 | 0.5 | 0.009 | 0.004 | 0.01 | 0.9 | 180 |
| Cranium | 0.0014 | 0.0003 | 0.01 | 0.1 | 0.0036 | 0.0001 | 0.01 | 0.4 | 257 |
| Mandible | 0.136 | 0.003 | 0.01 | 13.6 | 0.135 | 0.008 | 0.01 | 13.5 | 99 |
| Cervical spine | 0.132 | 0.001 | 0.01 | 13.2 | 0.0425 | 0.0001 | 0.01 | 4.3 | 32 |
| Thyroid | 0.03 | 0.001 | 0.04 | 12.0 | 0.04 | 0.02 | 0.04 | 16.0 | 133 |
| Parotid | 0.123 | 0.003 | 0.01 | 12.3 | 0.146 | 0.004 | 0.01 | 14.6 | 119 |
| Average child/adult | 137 | ||||||||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


