In many ways, autogenous bone grafts continue to remain the gold standard for repair of jaw atrophy and bone defects. Autogenous bone grafting is a well-documented procedure for reconstruction of the atrophic maxilla and mandible for rehabilitation with implant prostheses. Advancements in biologic engineering will produce alternatives to autogenous bone that may very well exceed existing clinical outcomes and replace traditional indications for its use. However, the increased costs of technology can be an obstacle to routine use of new products. Autogenous bone grafting offers a well-proven, predictable method for ridge augmentation and defect repair for dental implant placement.
The use of autogenous bone with dental implants was originally discussed by Branemark et al. Early studies focused on the use of iliac bone grafts in the treatment of the atrophic, edentulous maxilla and mandible. Although the iliac crest is most often used for major jaw reconstruction, it has the disadvantages of the need for hospitalization, general anesthesia, and alteration of ambulation. Additional donor sites have been evaluated, including the calvarium, proximal tibia, and maxillofacial regions. Autogenous bone can be used in several forms, including cancellous marrow, particulate bone chips, or cortical and corticocancellous blocks. The timing of graft placement and implant insertion has been well researched. The preferred approach in most cases today is delayed implant placement into the healed bone graft. Earlier studies of machined screw type of implants often found lower survival rates in grafted bone. The use of implants with enhanced surface features has improved outcomes in regenerated bone, with success rates comparable with those in native bone.
▪
BONE BIOLOGY
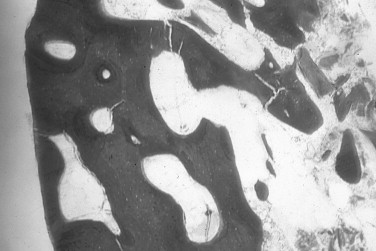
Autogenous bone is the only graft material with osteogenic properties that can directly form bone. Bone cells, in higher concentration in the cancellous marrow, surviving the transplantation produce new bone. In addition, bone morphogenetic proteins and growth factors are present within the autograft that induce bone formation in the surrounding tissues. Osteocompetent mesenchymal cells are transformed into osteoblasts through osteoinduction. The cortical portion of the autogenous bone graft acts as an osteoconductive scaffold for bone formation. The graft is remodeled and replaced with new bone over time (creeping substitution) ( Figure 24-1 ). Free autogenous bone grafts must become revascularized to incorporate into the recipient bed. The cancellous portion of the graft revascularizes faster than the cortex. The denser cortical bone revascularizes through its existing haversian system.
The subject of embryologic origin of autologous bone grafts has received much attention regarding graft incorporation and resorption. Membranous bone grafts, from the mandible or calvarium, have been found to reveal less resorption than grafts from endochondral sites, such as the iliac crest. Most studies examining the influence of graft origin on resorption refer to onlay augmentation with block bone grafts. It is important to make a distinction between the graft morphology (particulate, block) and whether the graft is used for onlay or interpositional placement. Interpositional bone grafts typically resorb less bone than is used for onlay augmentation. Sinus floor augmentations are more comparable with interpositional rather than onlay bone grafts, and therefore less resorption would be expected. More recent studies examining graft loss have challenged the hypothesis of embryologic origin and emphasize the microarchitecture of the bone used for grafting. Ozaki and Buchman found that regardless of their embryologic origin, cortical bone grafts reveal less volume loss than cancellous bone grafts. Cortical bone grafts from the mandible exhibit minimal resorption and maintain their dense quality, making them ideal for onlay augmentation before implant placement ( Figures 24-2 , 24-3 ).


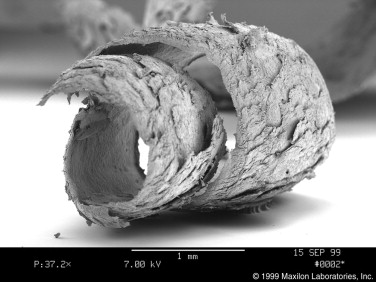
Following harvest, the bone graft should immediately be stored in sterile saline to maintain cellular vitality, and minimal time should elapse between graft procurement and placement. However, the number of viable cells contained in mandibular cortical grafts is probably insignificant in new bone formation. If block grafts or trephine cores are milled into particulate bone, the particle size should not be too fine. Some burs or mills pulverize the bone graft into a powder or paste. Whereas bone powder is quickly resorbed, slightly larger particles are more osteoconductive and act as a better scaffold for bone formation. The other potential disadvantages of bone powder collected by a suction trap include the negative effects of heat generated in bone preparation and desiccation of the particles. Bone scrapers produce ribbonlike shavings that have a favorable three-dimensional morphology for revascularization and graft incorporation ( Figure 24-4 ).
The addition of supplemental autologous growth factors, such as platelet-rich plasma, has been reported to enhance and accelerate the incorporation of autologous cancellous bone grafts. In addition, platelet-rich plasma may be useful as a matrix for soft tissue repair, adhesive of bone graft particles, and for improving surgical hemostasis ( Figure 24-5 ). Adding a prepared concentrate of the patient’s platelets to the bone grafted site can also enhance and accelerate soft tissue wound healing. The various cytokines and mediators found in the alpha granules of the platelets promote angiogenesis and collagen synthesis. This may diminish the risk of wound dehiscence and bone graft exposure to the oral cavity.

▪
PREOPERATIVE EVALUATION
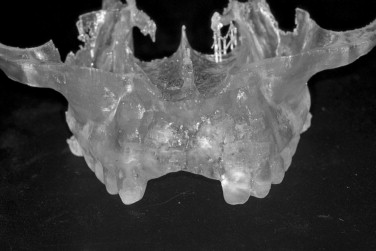
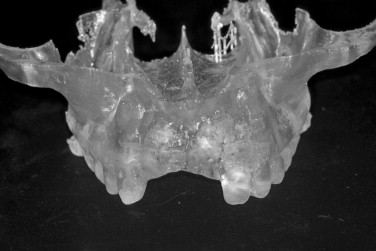
A comprehensive evaluation of the graft recipient site is necessary for planning of the bone graft surgery. Panoramic and periapical radiographs are used to evaluate the bone defect, surrounding dentition, and regional anatomy. Computed tomography (CT) is useful for three-dimensional views of the bone deficiency and can also be used to assess intraoral donor sites. Implant planning software can be used with the scan to more precisely evaluate the reconstructive needs of the patient ( Figure 24-6 ). A stereolithographic model of the jaw can be generated from the scan to further plan the case ( Figure 24-7 ). Mounted study casts and diagnostic waxing allow the clinician to better appreciate the ridge morphology in relationship to planned prosthetic outcome ( Figure 24-8 ). They also may be used for the fabrication of a radiographic template worn during the CT scan. The template reveals the radiopaque outline of the prosthetic tooth position in the tomographic view of the residual ridge. This allows a determination of graft size requirements and donor site options. A template of the planned prosthetic tooth position is also helpful for use during graft surgery to confirm graft positioning and fulfillment of the grafting requirements.


Treatment of the anterior maxilla requires an aesthetic zone evaluation. This includes determination of the high lip line and need for lip support. A diagnostic wax up will help determine tooth length and need for vertical augmentation to develop the correct tooth size. An emphasis must be placed on creating adequate osseous volume for implant placement and providing a proper soft tissue profile for the implant restoration.
The soft tissue character should be assessed, including quantity of keratinized tissue, thickness of the mucosa, muscle attachments, and the presence of scar tissue. It is often better to correct soft tissue problems before bone grafting. The lack of keratinized tissue in a region is best treated with autogenous free gingival grafting ( Figures 24-9, 24-10, 24-11 ). Areas of thin alveolar mucosa can be enhanced with the interpositional placement of allogeneic dermis or connective tissue grafts. The removal of scar tissue improves blood supply to the area and helps improve the mobility of the soft tissue flap over the bone graft. The removal of a frenum or high muscle attachments in the recipient site will reduce tension on the incision line. Soft tissue corrective surgery should be performed at least 8 weeks before bone graft surgery to allow incorporation of any grafts and reestablishment of vascularity to the area.



The periodontal health and endodontic status of teeth adjacent to the graft recipient site should be evaluated before grafting. It may be prudent to extract hopeless teeth before grafting, especially if infection is present. The marginal bone height on the teeth bordering the bone defect determines the level that may be achieved with vertical bone augmentation. It may be necessary to extract stable teeth if they have bone loss that limits the augmentation requirements.
▪
PREOPERATIVE EVALUATION
A comprehensive evaluation of the graft recipient site is necessary for planning of the bone graft surgery. Panoramic and periapical radiographs are used to evaluate the bone defect, surrounding dentition, and regional anatomy. Computed tomography (CT) is useful for three-dimensional views of the bone deficiency and can also be used to assess intraoral donor sites. Implant planning software can be used with the scan to more precisely evaluate the reconstructive needs of the patient ( Figure 24-6 ). A stereolithographic model of the jaw can be generated from the scan to further plan the case ( Figure 24-7 ). Mounted study casts and diagnostic waxing allow the clinician to better appreciate the ridge morphology in relationship to planned prosthetic outcome ( Figure 24-8 ). They also may be used for the fabrication of a radiographic template worn during the CT scan. The template reveals the radiopaque outline of the prosthetic tooth position in the tomographic view of the residual ridge. This allows a determination of graft size requirements and donor site options. A template of the planned prosthetic tooth position is also helpful for use during graft surgery to confirm graft positioning and fulfillment of the grafting requirements.


Treatment of the anterior maxilla requires an aesthetic zone evaluation. This includes determination of the high lip line and need for lip support. A diagnostic wax up will help determine tooth length and need for vertical augmentation to develop the correct tooth size. An emphasis must be placed on creating adequate osseous volume for implant placement and providing a proper soft tissue profile for the implant restoration.
The soft tissue character should be assessed, including quantity of keratinized tissue, thickness of the mucosa, muscle attachments, and the presence of scar tissue. It is often better to correct soft tissue problems before bone grafting. The lack of keratinized tissue in a region is best treated with autogenous free gingival grafting ( Figures 24-9, 24-10, 24-11 ). Areas of thin alveolar mucosa can be enhanced with the interpositional placement of allogeneic dermis or connective tissue grafts. The removal of scar tissue improves blood supply to the area and helps improve the mobility of the soft tissue flap over the bone graft. The removal of a frenum or high muscle attachments in the recipient site will reduce tension on the incision line. Soft tissue corrective surgery should be performed at least 8 weeks before bone graft surgery to allow incorporation of any grafts and reestablishment of vascularity to the area.



The periodontal health and endodontic status of teeth adjacent to the graft recipient site should be evaluated before grafting. It may be prudent to extract hopeless teeth before grafting, especially if infection is present. The marginal bone height on the teeth bordering the bone defect determines the level that may be achieved with vertical bone augmentation. It may be necessary to extract stable teeth if they have bone loss that limits the augmentation requirements.
▪
PATIENT PREPARATION
Patients undergoing autogenous bone grafting require antibiotic prophylaxis. The antibiotic of choice for most cases is amoxicillin. For patients allergic to amoxicillin, either a cephalosporin or clindamycin may be considered. Antibiotics should be administered before surgery to obtain proper blood levels and continued for 1 week. The use of short-term glucocorticoids can diminish postoperative facial swelling, local flap edema, and discomfort. Narcotic analgesics are prescribed for use during the immediate postoperative course. Thereafter, the patient may transition into the use of nonsteroidal antiinflammatory medications. Some studies have found bacterial contamination of orally harvested bone grafts, especially when suction traps are used to collect drilled bone debris. Chlorhexidine rinsing before surgery has been shown to significantly reduce this problem. Preoperative antisialagogue agents, such as glycopyrrolate, are also useful to decrease salivary flow, which may carry bacteria into the graft site. Aseptic surgical technique should be maintained because these reconstructive procedures are more involved and may often require more operative time. Most cases involving autogenous bone grafting in the office are performed under intravenous anesthesia. Shorter, less involved graft procedures may be treated using oral sedation techniques.
▪
BONE GRAFT DONOR SITES
MAXILLARY TUBEROSITY
Although the maxillary tuberosity offers a smaller amount of bone than other donor sites, the softer consistency of the graft is often favorable for filling bone defects. The bone in the tuberosity area is porous, and the outer cortical layer is thin. Because the tuberosity is in the same surgical field when performing a lateral approach to sinus grafting, it should be routinely considered for bone harvest. The amount of bone that may be obtained can be deceiving because the mucosa over the tuberosity is usually much thicker. A periapical or panoramic radiograph can be used to better assess the underlying bone. CT of the maxillary sinus region can allow threedimensional quantification of the area. The anatomic limitations of tuberosity bone harvest include the maxillary sinus, pterygoid plates, molar teeth, and the greater palatine canal. To gain access to the area for bone harvest, an incision is made along the ridge crest over the tuberosity. A vertical releasing incision is made along the lateral aspect of the posterior maxilla. Mucoperiosteal reflection exposes the tuberosity, ridge crest, and lateral maxilla. The palatal tissue should also be elevated to reveal the entire width of the tuberosity. The graft may be harvested with a chisel or rongeurs ( Figures 24-12 , 24-13 ). The chisel edge should be kept slightly superficial to the maxilla to shave off pieces of tuberosity bone and prevent inadvertent sinus communication. A chisel can also be used along the posterior lateral maxilla to obtain a thin piece of cortical bone, used to cover the window following grafting of the sinus floor.


MANDIBULAR SYMPHYSIS
The symphysis of the mandible has been used extensively for sinus and onlay bone grafting. *
*
Techniques to harvest block or particulate bone grafts from the anterior mandible have been reported. The symphysis donor site offers the greatest volume of intraoral bone. The average interforaminal distance is approximately 5.0 cm, and the depth of the anterior mandible usually exceeds 1.0 cm. A CT scan or panoramic radiograph is used to evaluate the available bone in this donor site. A lateral cephalometric radiograph can be useful to determine the anteroposterior dimension of the anterior mandible. Periapical radiographs give a more accurate measurement of the tooth root lengths.
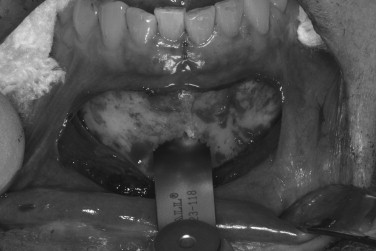
The ease of surgical access is one of the main advantages of the symphysis region. Bilateral mandibular blocks and local infiltration in the anterior mandible are administered using 2% lidocaine, 1 : 100,000 epinephrine. Exposure of the symphysis may be obtained through a sulcular or vestibular incision. The vestibular incision is made in the mucosa between the cuspid teeth, approximately 1 cm from the mucogingival junction. Limiting the distal extent of the incision will reduce the risk of mental nerve injury. A vestibular approach allows easy access, but produces more soft tissue bleeding and possible intraoral scar formation. The sulcular approach should not be used when mucogingival defects are present and may result in gingival recession. The sulcular incision should extend to the premolar regions bilaterally. A mucoperiosteal flap is reflected to expose the mental foramina and the inferior border of the mandible (pogonion). Additional local anesthesia is often needed at the base of the mandible to block cervical innervation.
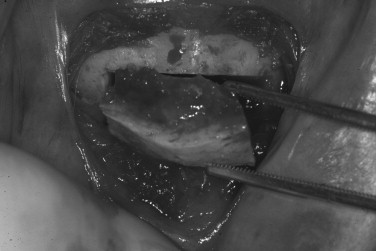
After the symphysis region is exposed, the osteotomies for graft harvest are planned. The dimensions of the graft are determined by the bone volume necessary to reconstruct the recipient site. Osteotomies should be kept at least 5 mm from the root apices and the mental foramina. In most cases, the inferior and lingual cortices of the mandible are left intact. The facial cortex is thick, and the underlying cancellous bone is usually dense. The osteotomies may be made with a carbide fissure bur (#557 or 701) in a surgical hand piece or sagittal saw ( Figures 24-14 , 24-15 ). Following an osteotomy through the outer cortex and into the cancellous bone, the graft is removed with a chisel. A unibeveled chisel is tapped along the osteotomies, with the exception of the inferior border, to fracture the block from its base ( Figure 24-16 ). The block bone graft may also be harvested in segments by sectioning the rectangular piece in the midline. Two bone blocks are often easier to harvest because the second block can be fractured from its lingual base with the chisel. Some additional cancellous bone may be procured with a curette, chisel, rongeur, or trephine after the block is removed, but the volume is meager. Following the removal of the block graft, hemostatic materials, such as collagen or gelatin, may be placed over the cancellous bone. When larger bone grafts are harvested, the donor site should be filled with a bone substitute, such as resorbable hydroxyapatite, to maintain facial contour. Smaller or particulate bone grafts may be procured using trephine burs, bone collection traps, or bone-scraping instruments. Closure of the donor site is typically performed after the graft is inserted into the recipient site. This minimizes the time between graft harvest and placement. The mucosa superior to the vestibular incision is reflected to reduce tension on the flaps from edema and lip movement. The vestibular incision is closed in layers using resorbable sutures. The deeper layers may be sutured with 4-0 Vicryl, and the superficial mucosa can be closed primarily with 4-0 chromic gut. Postoperative pressure dressings are used over the chin to reduce edema, hematoma formation, and incision line opening.

The mandibular symphysis is associated with a higher incidence of postoperative complications than other maxillofacial donor sites. Altered sensation of the lower anterior teeth is a relatively common postoperative symptom when bone blocks or trephine cores are removed. The contents within the incisive canal of the symphysis that innervate the teeth are disrupted during bone harvest. Patients describe dullness in sensation of the incisors, which usually resolves within 6 months. The need for endodontic treatment of anterior teeth is very rare. Neurosensory disturbances in the chin region also may be encountered, even when a sulcular incision is used. The incidence of temporary mental nerve paresthesia for symphysis graft patients is usually low, but has been found to be as high as 43%. Meteorotropism of the chin has also been reported. Although the vast majority of these nerve injuries recover, they are disconcerting to patients. It is prudent to discuss the possibility of temporary altered sensation of the teeth and chin before surgery. Although no postoperative alteration in soft tissue chin contour has been reported, patients are often concerned with the possible aesthetic consequences of bone removal from this area. Radiographic evidence of incomplete bony regeneration has been reported in elderly patients. Filling the donor site with a resorbable bone substitute, such as bank or bovine bone, can help alleviate the patient’s concerns. Ptosis of the chin has not occurred and can be prevented by avoiding complete degloving of the mandible. As there is greater morbidity associated with harvesting chin bone, this donor site is usually reserved for cases requiring greater graft thickness than the ramus can offer (greater than 4.0 mm) ( Figures 24-17 through 24-21 ).





MANDIBULAR RAMUS
The posterior mandible is an excellent donor site for bone harvest, and this region offers several advantages over the symphysis. A CT scan or panoramic radiograph is used to evaluate the bony anatomy, including the ramus, external oblique ridge, and mandibular canal. A mandibular block and buccal infiltration in the posterior mandible is administered using 2% lidocaine, 1 : 100,000 epinephrine. The incision design for access to this region differs for block and particulate bone harvest. When taking a block graft, the incision is made similar to one used in third molar removal. A sulcular incision is made along the posterior teeth. The incision is continued posteriorly and lateral at a 45-degree angle from the distobuccal aspect of the second molar or the base of the retromolar pad if no molar is present. The incision extends superiorly along the ascending ramus. Following the incision, a mucoperiosteal flap is reflected to expose the lateral ramus and body of the mandible. The masseter muscle is reflected laterally with a large retractor to form a large open pocket. Additional local anesthesia is often required in this area to block cervical innervation. The limits of the ramus area are dictated by clinical access in addition to the coronoid process, molar teeth, and inferior alveolar canal. The average anteroposterior dimension of the mandibular ramus is 30.0 mm, and the lingula is typically in the posterior third.
Four osteotomies are made to harvest a block bone graft—external oblique, superior ramus, anterior body, and inferior ( Figure 24-22 ). The length of the osteotomies is determined by the bone volume necessary to reconstruct the site. The cortical cuts are made with a carbide fissure bur (#557 or 701) in a straight hand piece under sterile saline irrigation. The external oblique cut is made along the anterior border of the ramus, approximately 4.0 to 6.0 mm medial to the external oblique ridge. This osteotomy can extend as high as the base of the coronoid process and anteriorly up to the first molar area. This can produce a graft that may approach up to 40.0 mm in length. The superior ramus cut is made through the lateral cortex of the ramus and perpendicular to the external oblique cut. It may extend as far posteriorly on the ramus as the opposing lingula on the medial ramus. However, the length of this cut is typically about 10.0 mm. The anterior body cut may often extend over the path of the mandibular canal. Although the buccolingual position of the mandibular canal is variable, the distance from the canal to the medial aspect of the buccal cortical plate (medullary bone thickness) was found to be greatest at the distal half of the first molar (mean: 4.05 mm). Therefore, the anterior body cut should be made in this area and not in the third molar region, where the canal is closer to the buccal surface. This anterior body cut is progressively deepened until bleeding from the underlying cancellous bone is visible. The inferior osteotomy is only a partial-thickness cut made with a round carbide bur (#8). It connects the inferior aspects of the superior ramus and anterior body cuts. This osteotomy on the lateral aspect of the ramus parallels the external oblique cut and creates the base of the rectangular bone block. It extends only partially through the cortex and creates a line of fracture. The block graft is then removed with a chisel wedged within the external oblique osteotomy. Care should be taken to parallel the chisel with the lateral surface of the mandible and limit the depth of penetration. An alternative technique is to insert an extraction elevator and pry the graft free ( Figure 24-23 ). This donor site is not augmented with bone substitutes because the inferior alveolar nerve may be exposed and irritated by the graft particles. The incision is closed primarily with resorbable sutures (4-0 chromic gut). A rectangular piece of bone approximately 4.0 mm in thickness may be harvested from the ramus ( Figure 24-24 ). This morphology is well suited for veneer grafting to gain additional ridge width or the block may be particulated in a bone mill.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


