Introduction
Head and neck skeletal anomalies or normal variants might predict the occurrence of palatally displaced impacted maxillary canines. Despite their clinical importance, studies in this regard are rare, especially when it comes to vertebral anomalies.
Methods
This case-control study was performed on cephalographs of 35 orthodontic patients (11 male, 24 female) with palatally displaced canines (PDC) and 75 patients without them (29 male, 46 female). PDC were diagnosed on panoramic and lateral cephalographs and from clinical reports. The occurrence and severity of sella turcica bridge and the atlas ponticulus posticus, and deficiency of the posterior atlas arch were evaluated twice on lateral cephalographs. The associations between the occurrence and level of these skeletal anomalies and variations of PDC occurrence as well as additional correlations were assessed using multivariable and bivariate statistics (α = 0.05; β ≤0.2).
Results
The patients’ mean age was 18.4 ± 1.9 years. In the control and patient groups, 23 (30.7%) and 21 subjects (60%) had sella turcica bridging, respectively (chi-square, P = 0.003). Ponticulus posticus was observed in 14 (18.7%) controls and 15 (42.9%) patients (chi-square, P = 0.007). Posterior atlas arch deficiency was observed in 4 (5.3%) controls and 5 (14.3%) patients (chi-square, P = 0.111). The presence of ponticulus posticus and sella turcica bridging might be associated with increased odds of PDC occurrence for about odds ratios of 3.1 and 3.5 times, respectively (binary logistic regression).
Conclusions
PDC is positively associated with the occurrence and severity of sella turcica bridging and ponticulus posticus. The association between PDC and posterior atlas arch deficiency was inconclusive.
Highlights
- •
Palatally displaced canine (PDC) impaction is associated with sella turcica bridging.
- •
PDC occurrence is associated with atlas arcuate foramen (ponticulus posticus) development.
- •
Severity of sella turcica bridging might be associated with ponticulus posticus development.
Maxillary canine impaction is a common dental anomaly found in 1.1% to 13% of the population, with a higher prevalence in female patients. Common theories contributing to the etiology of maxillary canine impaction are the guidance and genetic theories. The guidance theory suggests that local mechanical factors interfere with the path of canine eruption as potential etiologies. According to the genetic theory, impacted maxillary canines are conjointly associated with other genetic abnormalities such as submerged deciduous molars, hypoplastic enamel, mandibular premolar aplasia, and diminutive maxillary lateral incisors. Palatally displaced canines (PDC) can cause numerous clinical problems such as midline shift, root resorption, and malocclusion; also, their treatment is more difficult and expensive in older patients. Early diagnosis and timely intervention of impacted canines might reduce the time, cost, and complexity of treatment.
Conventional imaging is routinely used in orthodontics for various purposes, including diagnosing the position and the expected path of eruption of the permanent canines. Cephalometric radiographs are used to evaluate the development, growth, and morphometric relationships of craniofacial and dental structures, but they also include other diagnostic information about the skull, face, and upper cervical spine occurring with craniofacial and dental deviations. Some of these might be valuable for an early diagnosis of a developmental problem. The calcification of the sella turcica bridge might be positively associated with PDC. The reason might be that sella turcica, dental epithelial progenitor cells, and maxillary, palatal, and frontonasal developmental fields share a common embryologic origin (neural crest cells). In addition, genetic mutations might negatively influence the development of the midface, teeth, and parts of the sella turcica.
However, the only reason they are of interest is not to assist in detecting PDC. The neural crest might play a role in neck and shoulder skeletal development, sella turcica bridging, and dental development and eruption. Anomalies of the cervical vertebrae might be associated with malformations of the jaw, condyle, and craniofacial morphology, occlusion, and tooth anomalies or might cause clinical problems. Therefore, their assessment might provide useful clinical information regarding the health of other organs and craniofacial structures. Of these skeletal features, 3 (sella turcica bridging, deficiency of the posterior arch of the atlas vertebra, and sagittal atlas foramen [or ponticulus posticus]) are available radiographically.
Sella turcica bridging is a frequent morphologic variation (1.1%-22%), caused by excessive ossification of the dura mater between the posterior and anterior clinoidal processes of the sphenoid, or caused by an abnormal embryologic development of the sphenoid. The sella turcica bridge might be associated with multiple craniofacial or systemic developmental syndromes and disorders as well as numerous local dental anomalies such as tooth transpositions and congenitally missing teeth. The ponticulus posticus (also called the sagittal or arcuate foramen) is a frequent (5.14%-37.83%) abnormal bony prominence. It arises from the superior articulating process of the atlas, encircles the vertebral artery completely or partially, and reaches the atlas posterior arch. It can cause or be associated with numerous clinical problems. The atlas posterior arch can itself be deficient in fewer than 5% of normal people. Although it is usually silent clinically, it also can be associated with clinical symptoms and problems.
Despite the clinical implications of these common radiographic features, evidence regarding associations between these skeletal anomalies and variants and the occurrence of PDC is scarce. Only 3 studies are available regarding the associations between PDC and sella turcica bridging, with 1 study regarding PDC association with ponticulus posticus and posterior arch deficiency. Moreover, the correlations between these skeletal anatomic features have not been assessed before. Hence, we aimed to investigate the predictive value of these skeletal anomalies. As additional findings, we also evaluated the roles of sex, age, and Angle occlusion classes in predicting PDC and the 3 skeletal anomalies. The null hypotheses were as follows. There would be no associations (1) between the skeletal anomalies and PDC, (2) among the 3 skeletal anomalies, and (3) among age, sex, and Angle occlusion classes with PDC and the skeletal anomalies.
Material and methods
This case-control study was performed with 110 pretreatment lateral cephalometric radiographs of 2 groups. The patient group consisted of 35 orthodontic patients with PDC. The control group consisted of 75 orthodontic patients with normally erupted canines. At least 35 subjects in the control group (n = 75) were age- and sex-matched with the 35 patients. The subjects were treated ethically, and the protocol was approved by the institutional review board of Islamic Azad University; no personal patient information was collected. All patients in both groups were from 1 city (Tehran, Iran) and the same ethnic background (white people of Iranian ancestry).
To collect the patient group, all pretreatment radiographs of an orthodontic department and a private dental clinic (more than 800 radiographs) were searched randomly until the desired number of cephalographs (patients with PDC) were approved according to the eligibility criteria. Cephalographs of normal patients (without PDC) were randomly selected from the remainder of the radiographs until the predetermined sample size was reached.
For each patient with PDC, there was at least 1 same-sex, same-age control subject without PDC. The exclusion criteria comprised incomplete patient files (incomplete information or lacking either panoramic or lateral cephalograph images and orthodontic diagnostic casts), poor image qualities, nonstandardized cephalographs (eg, not depicting any regions of interest), any syndromes or systemic diseases, any severe mandibular deviation, trauma history, or any head and neck surgery histories, any history of radiotherapy or chemotherapy, any orthodontic treatments or surgeries, and any dental anomalies (of size, shape, or number) except PDC, which was acceptable only for the patient group. No patient had any history of cardiovascular or lung diseases, anemia, jaundice, allergies, and current medication consumption.
The inclusion criteria were age of 14 years or older and preferably less than 21 years (since canine development usually finishes at 12 or 13 years of age). In addition, the images of the atlas and sella turcica needed to be clearly visible in the radiographs. To be included in the patient group, subjects needed to have at least 1 maxillary PDC (with any depth, position, direction, or severity). To be included in the control group, subjects needed to have no dental anomalies at any degree of severity (even very mild).
Palatally impacted canines were diagnosed using dental panoramic and lateral radiographs as well as every other available source of information (ie, cone-beam computed tomography, patient files and records of clinical diagnosis of PDC, and directly asking the patients’ orthodontists). The side and number of impacted canines per patient were recorded.
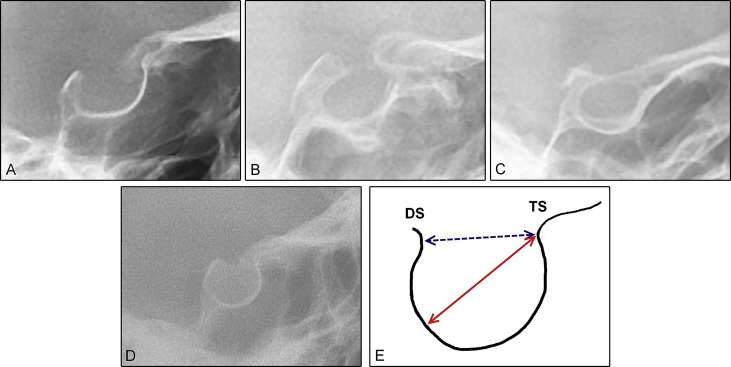
For sella turcica bridging (calcification), all cephalographs were traced manually using conventional methods on acetate sheets with a 0.5-mm lead pencil in a dark room. Sella turcica was drawn as a U-shaped structure from to the tip of the tuberculum sellae to the tip of the dorsum sellae visible on the radiograph. The linear dimensions were measured as follows.
- 1.
Interclinoidal distance (sella length): the distance from the tip of the tuberculum sellae to that of the dorsum sellae.
- 2.
The greatest anteroposterior diameter of sella: the longest distance between the tip of the tuberculum sellae and the posterior contour of sella.
To quantify the severity of bridging, the standard scoring scale developed by Leonardi et al was applied: no calcification or bridging (normal sella, type I); the interclinoidal distance (sella length) was either equal to or greater than 3 quarters of the greatest anteroposterior diameter. Partial calcification (type II): the interclinoidal distance was equal to or less than 3 quarters of the greatest anteroposterior diameter. Complete calcification (type III): only the diaphragm sellae was evident on the radiograph ( Fig 1 )
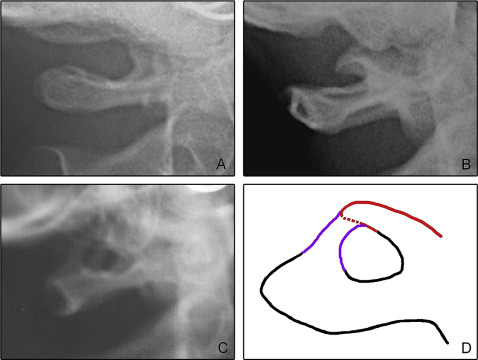
The extent of developed ponticulus posticus on the atlas was estimated as none (no bony emergence was observed), incomplete (partial bony emergence), or complete (complete bone bridge was observed, Fig 2 ).
The completion of the posterior arch of atlas was also evaluated by the same observer (M.H.G.) ( Fig 3 ).

The Angle classes were determined based on the patients’ clinical reports (assessed by their orthodontists, using bite registration waxes) and orthodontic diagnostic casts.
After about 2 years, all images, casts, and records were reevaluated by the observer. There were above 95% intraobserver agreements for PDC occurrence, posterior arch deficiency, ponticulus posticus development, sella turcica bridging (all binary variables), and occlusion (all 5 P values = 0.000). One year later, another examiner evaluated 30 randomly selected radiographs and patient files regarding these variables except for the occlusion. The interobserver agreements were 100% for PDC occurrence and above 80% for the skeletal anomalies.
Statistical analysis
The sample size sufficed to provide test power above 80% for comparisons of sella turcica bridging. Descriptive statistics were calculated. The groups’ ages and sexes were assessed using chi-square tests and independent-samples t tests. The associations between the occurrence of PDC with each variable, sella turcica bridging, posterior arch deficiency, and ponticulus posticus development, were assessed using a chi-square test. In addition, the associations among the variables occlusion, age, sex, PDC, sella turcica bridging, ponticulus posticus development, and posterior atlas arch deficiency’ were evaluated. The associations of all variables with PDC were evaluated using multiple binary logistic regression analyses. Odds ratios (OR) and 95% confidence intervals (CI) were calculated. The level of significance was set at 0.05.
Results
Sample characteristics are summarized in Table I .
| Parameter | Patient | Control | P |
|---|---|---|---|
| Sex | 11 male | 29 males | 0.462 (chi-square) |
| 24 female | 46 female | ||
| Age (y) | 18.7 ± 1.6 | 18.2 ± 2.0 | 0.190 ( t test) |
| Canine impaction | 23 (65.7%) unilateral | None | – |
| 12 (34.3%) bilateral | |||
| Angle Class | 21 (60%) I | 47 (62.7%) I | 0.843 (chi-square) |
| 13 (37.1%) II | 27 (36%) II | ||
| 1 (2.9%) III | 1 (1.3%) III |
In the control group, 23 subjects (30.7%) had sella turcica bridging (types II and III according to Leonardi et al ), and 21 subjects (60%) in the patient group had this anomaly (types II and III combined). The difference between the 2 groups was statistically significant (chi-square, P = 0.003).
Of the 75 control subjects, 52 (69.3%), 19 (25.3%), and 4 (5.4%) had types I (normal sella [no bridging]), II, and III of sella turcica calcification. However, 14 (40.0%), 16 (45.7%), and 5 (14.3%) of the 35 PDC patients had types I, II, and III of sella calcification. According to the chi-square test, the distributions of sella calcification types differed between the 2 groups ( P = 0.012).
Sella turcica bridging (types II and III combined) was observed in 23 female (32.9%) and 21 male (52.5%) subjects. This difference was significant (chi-square, P = 0.043).
Ponticulus posticus was observed in 14 (18.7%) control subjects and 15 (42.9%) patients, with a statistically significant difference (chi-square, P = 0.007). In the control group (n = 75), 61 (81.3%) did not have ponticulus posticuses, 10 (13.3%) had incomplete ponticulus posticuses, and 4 (5.4%) had complete ponticulus posticuses. Among the 35 patients, 20 (57.1%) did not have ponticulus posticuses, whereas 7 (20%) and 8 (22.9%) had incomplete and complete ponticulus posticuses, respectively. The chi-square test indicated a significant difference between the distributions of the 2 groups ( P = 0.010).
Posterior atlas arch deficiency was observed in 4 (5.3%) control subjects and 5 (14.3%) patients, with a marginally significant difference (chi-square, P = 0.111).
There was a significant positive correlation between sella turcica bridging and posterior arch deficiency (binary). No variable—canine impaction, sella turcica bridging, posterior arch deficiency, or ponticulus posticus—was correlated to Class I occlusion (all 4 P values ≥0.390) and Class II occlusion (all 4 P values ≥0.680). Class III occlusion was not associated with the variables canine impaction, posterior arch deficiency, and sella turcica bridging (all 3 P values ≥0.150). However, Class III was positively (although weakly) correlated with the occurrence and completion of ponticulus posticus (Spearman coefficient [ρ] = 0.229; P = 0.016).
The variables age, sex, occlusion type, sella turcica bridging (dichotomized), posterior arch deficiency (binary), and ponticulus posticus occurrence (dichotomized) were modeled in a logistic regression analysis ( Table II ). Only sella turcica bridging and ponticulus posticus occurrence were positively associated with impacted PDC ( Table II ). The presence of ponticulus posticus would increase the odds of palatally impacted canine occurrence by about 3 times (OR = 3.0). Also, sella turcica bridging increased this odds about 3 times (OR = 3.4; Table II ).


