Introduction
Despite the high prevalence of dental anxiety in children, there is little research examining anxiety before orthodontic procedures. This parallel-group randomized controlled trial assessed whether provision of additional multimedia information regarding the bond-up procedure affected anxiety in adolescent orthodontic patients. The effects of sex, ethnicity, and age were also investigated.
Methods
Participants were recruited from the orthodontic department of the Eastman Dental Hospital, University College London Hospitals Foundation Trust, in the United Kingdom; all were 10 to 16 years of age, with no history of orthodontic treatment, and patient assent and parental consent were obtained. The participants were randomized into control (n = 45) and intervention (n = 45) groups using a random number table. Both groups were given verbal information regarding the bond-up procedure, and the intervention group was additionally given a DVD showing a bond-up. Anxiety was assessed in the department immediately before the bond-up using the State-Trait Anxiety Inventory for Children, with state anxiety as the primary outcome measure. The researchers were unaware of group allocations while enrolling patients, scoring questionnaires, and analyzing data.
Results
A statistically significant difference was found between groups, with a difference in scores of 2 (95% confidence interval for the difference = 0.15 to 3.85). The median state anxiety was 32 in the control group (n = 42) and 30 in the intervention group (n = 43; P = 0.012). Sex, ethnicity, and age did not significantly affect anxiety. No harmful effects were noted.
Conclusions
Additional information reduces anxiety levels, but other methods could be more cost-effective than the DVD. Sex, ethnicity, and age did not statistically affect the anxiety levels.
Dental anxiety is a complex subjective emotion with many influencing factors: eg, age, sex, socioeconomic group, parental dental anxiety, and previous dental attendance and experiences. Studies show conflicting evidence with regard to the effects of these factors on anxiety. This is understandable when one considers the methodologic difficulties for researchers and the fact that it is not possible to objectively assess a patient’s own experience. Thus, patients must be relied upon to self-assess their anxiety; this introduces the possibility of reporting or recall bias. Recall bias can be reduced through the use of prospective trials; however, the assessment of an emotional response is complex. Several self-assessment tools have been developed for use in research into dental anxiety, but some are specific to general dental procedures (ie, restorative work or extractions); naturally, these do not apply to orthodontics.
Dental anxiety in children and adolescents is common and well documented, with direct repercussions on the care sought and received by patients. Despite the acknowledgment of the high prevalence of dental anxiety, there is currently little research examining anxiety levels before orthodontic procedures and methods for reducing it. Previous research has suggested that adolescent orthodontic patients are unclear about the process of placing fixed orthodontic appliances and would like more information to reduce their anxiety. The majority (87%) of participants in this research project stated that they thought that information in an audiovisual format would be beneficial because it would allow them to see what actually happens.
The reason for undertaking this study was therefore to examine the effect of additional multimedia information provision on anxiety levels in adolescent orthodontic patients before the bond-up procedure.
The aim of this study was to ascertain whether the additional preparatory information regarding the orthodontic bond-up procedure reduces anxiety in adolescent orthodontic patients. A secondary aim was to establish the influence of patients’ sex, ethnicity, and age on anxiety before the bond-up procedure.
The null hypotheses for this study were the following: (1) the provision of additional multimedia information regarding the orthodontic bond-up procedure does not affect the median anxiety score in adolescent orthodontic patients before the procedure; and (2) sex, ethnicity, and age do not influence the median anxiety score before the orthodontic bond-up procedure.
Material and methods
Ethical approval was obtained from the National Research and Ethics Service (reference number 11/LO/0392), and the University College London Hospitals Foundation Trust Research and Development Department granted research and development approval. This was a prospective parallel-group randomized controlled study in which patients were allocated into either the control or the intervention group. Verbal information regarding the bond-up procedure was provided by the treating orthodontist to the participants in both groups, according to the department’s usual practice. Patients in the intervention group were also given a DVD created specifically for this study and containing additional information regarding the bond-up procedure. Anxiety was assessed on the day of the procedure, just before the bond-up, using the State-Trait Anxiety Inventory for Children.
The patients for this study were recruited from the orthodontic department at the Eastman Dental Hospital, University College London Hospitals Foundation Trust, London, United Kingdom. They were 10 to 16 years old and were due to undergo fixed appliance treatment and able to give assent; parental consent was also obtained. Patients were excluded if they had a history of previous orthodontic treatment or were receiving other orthodontic interventions (eg, headgear) concurrently.
The participants were block randomized in groups of 10 to either the control or the intervention group using a random number table, with allocation of those with odd numbers to the control group and those with even numbers to the intervention group. To reduce bias, sealed opaque envelopes containing information relating to the allocations were prepared before the study. Since these were only opened once written consent and assent had been obtained, the researchers were not aware of the patient’s allocation while obtaining consent. The researchers remained blinded to group allocations when scoring the questionnaires and entering data into the results spreadsheet.
An Internet search was undertaken to assess the amount and quality of audiovisual information already available to patients and to establish whether any preexisting videos were suitable for use in this study. A number of videos concerning placement of fixed appliances were available; most were “homemade,” but some were commercial. However, several issues were noted, including the lack of verbal explanations, poor visibility of the actual procedure, and use of computer-generated models rather than a patient in some cases. A DVD was therefore created specifically for this study, with an introductory section explaining the components of a fixed appliance and the materials and instruments used during the procedure, followed by video footage of a patient having fixed appliances placed.
A trial DVD was created using footage of a colleague who was due to commence fixed appliance treatment and had consented to the filming of the bond-up for this purpose. This footage was edited to remove substantial repetitive scenes of the bond-up procedure because it was agreed that a viewer’s interest would not be maintained over a protracted time period. The footage was therefore edited until the DVD lasted 15 minutes. This draft was critiqued by the researchers, and changes were made to ensure that the explanation was more child friendly and the quality of the DVD footage was improved. It was also agreed that the patient shown in the video of the bond-up procedure should be in the same age group as those recruited for this study to allow effective “modeling.” Once a suitable patient had been identified and consented for the filming of the bond-up procedure, a second draft of the DVD was created. Again, this was appraised and edited until the researchers were satisfied that the DVD was as informative, engaging, and succinct as possible. DVD labels were then created to inform viewers that it should play automatically on insertion and to provide a contact e-mail address if they had any problems viewing the content.
The DVD was provided only to patients in the intervention group once written consent had been obtained and the group allocation had been checked. Because this was done before the bond-up date (eg, at the orthodontic records or treatment planning appointment), the patients could take the DVD home to watch before the bond-up appointment.
The outcome measure for this study was the patient’s anxiety score as measured by the State-Trait Anxiety Inventory for Children. Unlike some dental anxiety measurement tools, no scenarios are provided in this questionnaire. This, along with the fact that it was created specifically to measure anxiety in children and adolescents, makes it applicable for use in most medical and dental settings and ideal for this orthodontic study. This self-reported questionnaire comprises 2 scales to distinguish between state anxiety and trait anxiety. The state anxiety scale poses 20 questions, asking how respondents feel at that particular moment in time, thus assessing transitory anxiety states. The trait anxiety scale also asks 20 questions, but these relate to how the subject usually feels, thus assessing each patient’s relatively stable tendency to anxiety. Because information provision regarding a procedure is likely to affect anticipatory anxiety rather than the stable tendency to anxiety, the primary outcome measure was the state anxiety score.
The questionnaire was distributed to the patients by a researcher (J.P.K.S.) on the day of the bond-up procedure, immediately before their appointment. Each questionnaire had the patient’s unique identification number on the front page. The researcher provided verbal instructions about how to complete the questionnaire and highlighted the written instructions at the top of the questionnaire. An envelope was provided, and the patient was asked to seal the completed questionnaire inside and return it to the orthodontist or the reception staff. The patients were also asked to record on the outside of the envelope if they were in the intervention group but had not watched the DVD for any reason. The envelope was then returned to the researcher after the bond-up appointment, and the questionnaire was removed and placed into a file to be scored later. The outside of the envelope was checked for any notes before it was discarded. It was hoped that this method of collecting the questionnaires would reduce responder bias in patients who might have felt compelled to complete the questionnaire by selecting answers they perceived to be correct in the researcher’s eyes. Additionally, it was hoped that this assurance of anonymity would reduce any anxiety that the patients might feel if the completed questionnaire was visible to both researchers and clinicians whom they might expect to judge them on their responses.
Because there were no studies in the orthodontic literature with the same version of the State-Trait Anxiety Inventory for Children questionnaire, a sample-size calculation was carried out using data from the first 10 questionnaires returned from each group. The standard deviation of the state anxiety scores was 6.0, and the clinically relevant difference in state anxiety scores was set at 4.0 points. Using nQuery Advisor (version 4.0; Statistical Solutions Ltd, Cork, Ireland) and based on an independent 2-sample t test, it was estimated that 37 participants were required in each group for significance of P <0.05 and 80% power. Since the remaining results were unlikely to be normally distributed, it was probable that a Mann-Whitney U test would be used, so a correction factor was applied, resulting in a recommended sample size of 43 per group. To allow for dropouts from the study, it was decided that 45 participants should be recruited per group: ie, a total of 90.
The data were not normally distributed. To investigate differences between the control and the intervention groups, the median state, trait, and total anxiety scores were compared with the Mann-Whitney U test. This test was also used to investigate the effect of sex and ethnicity on anxiety. Univariable linear regression analysis was used to establish the independent effect of age on patient anxiety. It was thought that there might be a relationship between a patient’s underlying stable trait anxiety and how he or she reacts to stressful situations, and this might affect the analysis of the effect of information provision on anxiety. Therefore, a multivariable linear regression analysis was used to assess the group effect, with control for trait anxiety. The assumptions underlying the regression analyses were checked by a study of the residuals and found to be satisfied. A significance level of 0.05 was used for all hypothesis tests. All analyses were performed using SPSS software (version 21.0; IBM SPSS Statistics for Windows, Armonk, NY).
The mean state anxiety scores of both the male and female participants in this study were also compared with the normative values provided in the state-trait anxiety inventory for children manual, for the control and the intervention groups. A 1-sample t test was used for this comparison because the only normative values were mean values. Only state anxiety scores were compared because state anxiety scores had greater importance in this study.
Results
The participants were recruited between November 2011 and May 2012; 85 questionnaires were returned by December 2012. A CONSORT flow diagram ( Fig ) demonstrates the progression of patients in the study.
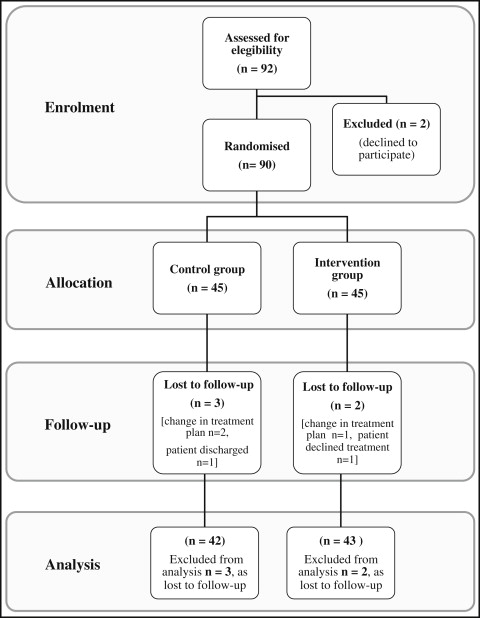
Of the 90 patients recruited, 85 returned to have fixed appliances placed and completed the questionnaire. Five patients were lost to follow-up, and the reasons included a change in treatment plan (n = 3), poor oral hygiene resulting in discharge (n = 1), and treatment declined (n = 1). The baseline demographics for the patients who completed the questionnaire are shown in Table I .


