Introduction
In nongrowing patients with skeletal Class II malocclusion, premolar extraction or maxillary distalization can be used as camouflage treatment. Zygomatic anchorage enables distalization in uncooperative or noncompliant patients. We describe 1 such procedure in a 24-year-old woman.
Methods
We used novel improved superelastic nickel-titanium archwires combined with nickel-titanium open-coil springs to provide a constant and continuous low force to the dentition.
Results
We were able to successfully eliminate the protrusive profile and correct the Class II molar relationship using this system of zygomatic anchorage. The posterior occlusal relationships were improved to achieve Class I canine and molar relationships on both sides, and ideal overbite and overjet relationships were established. Facial esthetics was improved with decreased protrusion of the upper and lower lips.
Conclusions
The method used here is a promising alternative to traditional distalization techniques and might offer an effective and simple means of distalizing maxillary molars in uncooperative patients.
Nonextraction treatment of Class II malocclusion in adult patients usually requires distal movements of the maxillary molars to establish Class I molar and canine relationships. However, distalization of the maxillary molars is difficult after complete eruption of the second molars in nongrowing patients. Moreover, maxillary unilateral molar distalization is more difficult than correcting a bilateral Class II relationship because the clinician must design an asymmetric force system.
Previous studies have reported unilateral molar distalization with the application of asymmetric facebows, improved Nance appliances, and the Keles slider. However, these appliances have disadvantages, such as their unesthetic appearance, loss of anchorage in the maxillary premolars, proclination of the incisors, relapse during retraction of the premolars and anterior teeth, undesirable intermittent forces, and dependence on patient cooperation. These treatment plans are thus unpopular with orthodontists.
To remedy the problems of noncompliance, intraoral distalizing mechanics combined with a skeletal anchorage system consisting of titanium anchor plates and monocortical screws has attracted attention. The implant anchor plate has been used as a multipurpose modality combined with a multibracketed appliance and enables movement of the maxillary molars distally without replacing the anchorage device during molar distalization. Furthermore, orthodontists can modulate the direction of force because the head portion is intraorally exposed and has 3 adjacent hooks for force adjustment.
Superelastic nickel-titanium wires have been widely used in clinical orthodontic treatment. These wires have many special properties including a shape-memory effect and superelasticity. Our department at Tokyo Medical and Dental University in Japan has developed an improved superelastic nickel-titanium wire and nickel-titanium open-coil spring that can generate orthodontic forces that vary minimally in response to changes in oral temperature.
In this case report, we describe the treatment of a woman with a skeletal Class II pattern and a unilateral Class II molar relationship using a system of zygomatic anchorage, and nickel-titanium alloy wires and open-coil springs.
Diagnosis and etiology
The patient was a 24-year-old woman with dental crowding and some difficulty in achieving lip closure. Pretreatment facial photographs show a convex profile and protrusion of the upper and lower lips, both of which exceeded the E-line (upper lip, 3.0 mm; lower lip, 4.5 mm) and were strained upon closure ( Fig 1 ). During lip closure, a mentolabial fold was observed in the chin area. A 1-mm deviation of the chin to the left of the midline was also evident. The right molar relationship was Class I, whereas the left molar relationship was Class II ( Fig 2 ). The maxillary midline deviated 1.5 mm toward the right, and the mandibular midline was 1.0 mm left of the facial midline.

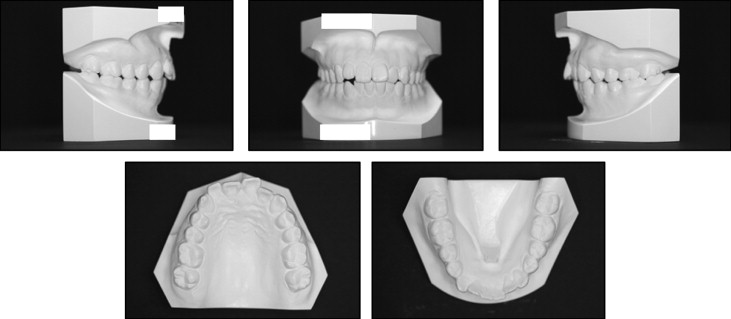
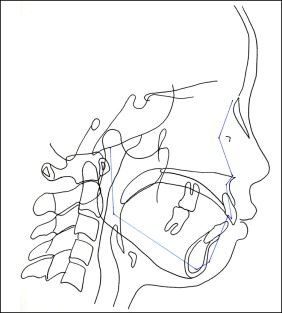
The patient had a 1-mm overbite and a 4-mm overjet. A pair of lateral and anteroposterior cephalometric radiographs and a dental panoramic radiograph were taken before treatment ( Fig 3 ). The cephalometric tracing ( Fig 4 ) and analysis ( Table ) demonstrated a Class II skeletal relationship (ANB, 4.5°) because of the retruded mandible. The SNA angle was within the normal range (79.6°), and the SNB angle was small (75.1°). The angle between the maxillary incisors and the SN plane was 105°, the mandibular incisor to mandibular plane angle was 106.9°, and the interincisal angle was 112.6°. The patient had a large tongue and a tongue thrust. Based on these findings, the patient was diagnosed as skeletal Class II with asymmetric molar relationships.

| Japanese norm | Pretreatment | Posttreatment | Retention | |
|---|---|---|---|---|
| SNA (°) | 82.3 ± 3.5 | 79.6 | 79.6 | 79.6 |
| SNB (°) | 78.9 ± 3.5 | 75.1 | 74.9 | 74.9 |
| ANB (°) | 3.4 ± 1.8 | 4.5 | 4.7 | 4.7 |
| FMA (°) | 28.8 ± 5.2 | 24.7 | 25.7 | 25.9 |
| U1-SN (°) | 104.5 ± 5.2 | 105.1 | 94 | 94 |
| IMPA (°) | 96.3 ± 5.5 | 106.9 | 102.7 | 102.7 |
| Interincisal angle (°) | 124.1 ± 7.6 | 112.6 | 126.3 | 126.5 |
Treatment objectives
The treatment objectives for this patient were to (1) relieve the crowding, which was her chief complaint; (2) eliminate the tongue thrust; (3) establish Class I molar and canine relationships; (4) correct the midline shift; (5) create ideal overbite and overjet; and (6) ultimately improve her facial profile.
Treatment objectives
The treatment objectives for this patient were to (1) relieve the crowding, which was her chief complaint; (2) eliminate the tongue thrust; (3) establish Class I molar and canine relationships; (4) correct the midline shift; (5) create ideal overbite and overjet; and (6) ultimately improve her facial profile.
Treatment alternatives
The patient had mandibular retrusion with lateral deviation. In growing children, orthopedic forces exerted by functional appliances can result in positive growth modification, which encourages growth of the mandible to correct the defect. In our adult patient, orthognathic surgical treatment was initially discussed as a means of correcting the skeletal discrepancy and the facial asymmetry, but this solution was rejected. For adults not wishing to undergo surgery, camouflage treatment with selective tooth extractions is a popular alternative. A nonsurgical approach with extraction of the maxillary first premolars and mandibular second premolars combined with the use of a transpalatal arch, J-hook headgear, or cervical headgear as anchorage for retraction of the anterior teeth is the traditional method. However, such methods carry a risk of reducing the space available for the tongue. This patient did not want any teeth extracted except for the third molars. Therefore, we extracted the third molars and chose the zygomatic anchorage as the approach for distalization.
Treatment progress
Before the orthodontic treatment, Y-shaped anchor plates (Orthoanchor SMAP; Dentsply-Sankin, Tokyo, Japan) were implanted onto the zygomatic process of the maxilla through the buccal mucosa under local anesthesia, and the maxillary and mandibular third molars were extracted. The plates were contoured to fit the bone surface. The head of the plate was intraorally exposed and positioned outside the dentition. After a month of healing, integration, and adaptation, 0.018 × 0.025-in slot preadjusted edgewise appliances (Sankin, Tokyo, Japan) were bonded to each tooth, and a 0.016 × 0.022-in improved superelastic nickel-titanium alloy wire (L & H Tomy, Tokyo, Japan) was used for the initial leveling.
During leveling of the posterior teeth, a nickel-titanium open-coil (100 g) spring was placed between the first molars and the second premolars to move the first and second molars distally, and a multibracket appliance was placed on the maxillary dentition ( Fig 5 , A ). During distal movement, a tie-back ligature wire was connected from the hook of the anchor plate to the power hook to eliminate the reciprocal force. At the same time, the mandibular right molars were uprighted with Class III elastics. Class III elastics were applied from the mandibular right first premolar to the anchor plate for 3 months ( Fig 5 , A ). After distal movement of the maxillary first and second molars, distal movement of the anterior segment was performed using sliding mechanics ( Fig 5 , B ). After space closure, distal apical movement was induced using an archwire with tip-forward bends ( Fig 5 , C ).


